Are you awake? Is your reality real? Are you sure?
Take the plunge down the rabbit hole of insanity and wonder in this fast-paced, nonstop psychological thriller that will leave you questioning the very nature of reality and beyond. Part thriller, part romance, part existential horror, A Dream of Waking Life delves into lucid dreaming, psychedelics, existential ontology, video games, the nature of love, the nature of reality, and more.
Outlast. Outgrow. Outlive. In the ashes of Earth, evolution is the ultimate weapon.
Mendel’s Ladder delivers an adrenaline-fueled journey set on a dystopian future Earth, brimming with high-stakes action, adventure, and mystery. This epic series opener plunges readers into a world filled with diverse cultures, heart-pounding battles, and characters who will captivate your heart and imagination.
Embark on a cosmic mystery spanning all of spacetime and beyond to discover the very nature of reality’s multilayered foundations.
“E.S. Fein is raising the bar for quality as it’s a very well-written and thought-provoking book…There are points and themes in the story that could be discussed for eons as people will have their own idea on where it leads. It’s a book I would highly recommend.” – Andy Whitaker, SFCrowsnest
This of course does not solely pertain to Chicagoans; any of you city slickers with those dark and snowy winters, those gloomy and menacing falls, and those extended rainy stormy weeks, are likely ignoring your immune system’s desperate cry for help. What am I doing wrong you may ask? What can I do when there is no sun to power me!? Even Superman was weak without the sun!
During the summer months in both hemispheres, influenza is virtually nonexistent. Aside from the flu, the common cold, which is actually a variety of more than 200 different viruses, also has a peak during the winter months.
Pish posh! I am 10 times the man I am during the winter period than the hot summertime! Look how efficiently I plow the snow and create icy sculptures with ease! I don’t need any supplements… John J. Cannell, MD, who heads the nonprofit Vitamin D Council, says otherwise:
Ninety-five percent of Americans are deficient in vitamin D — that’s how big the problem is
Ahh but there are always critics in the world of modern medicine. Why would anything natural and recurring in nature ever be good for you? All we need is antibiotics and drugs and we can solve the world’s problems! An article titled Trying to Avoid a Cold? Skip the Vitamin D Supplements, goes in detail describing how a study in New Zealand, not America, produced results that leave the reader questioning the validity of vitamin D benefits. Yet it notes that those deficient in vitamin D would still likely benefit from supplements. Look up to statistic… a flurry of brain synapses going off will ensue. For a time there was vitamin D hype, which brought on vitamin D hate, and now it is not even mentioned anymore. We can ride the news roller coaster and listen to the media until we are all completely confused about everything, even ourselves.
So how much should I take? Will I get poisoned from too much vitamin D?
The Vitamin D Council recommends that children take 1,000 IU and adults take 5,000 IU when not exposed to sunlight regularly. In order to reach a state of toxicity with vitamin D, one would have to consume over 40,000 IU in supplements for over two months! I have heard as little as 600 IU should be taken and if taken in excess of 1,000 IU then you risk toxicity. Boy do they steer us wrong about supplements, or as some call it, voodoo magic.
A little late, why didn’t you tell me this earlier!? Well better late then never.. SO! If it’s the summer time or spring time and you are actively soaking in your rays, safely of course without overexposure to damaging UV rays, then don’t sweat the vitamin D supplements as much! But if you do not eat vitamin D rich foods and you are prone to sickness and easily contract a flu during that dreaded FLU SEASON, do your immune system a solid and pop a supplement every now and then. Your body will repay you with longevity, energy, and a solid ‘D’ against that flu enemy!
• Allergies.Vitamin D deficiency is associated with a greater risk of allergies, such as to pollens.
• Back pain. Many studies have shown that in patients with chronic lower-back pain, vitamin D supplements led to either a partial or complete elimination of pain.
• Fibromyalgia. Low vitamin D levels are typical in this disease, and boosting vitamin D reduces symptoms.
• Heart disease.Low vitamin D levels are associated with up to a 50 percent higher risk of heart attack.
• Mental health. Low wintertime vitamin D levels may be a factor in seasonal affective disorder (that is, seasonal depression), as well as in schizophrenia.
• Multiple sclerosis. The risk of multiple sclerosis increases progressively in populations living at latitudes farther from the equator. A growing body of research suggests that adequate vitamin D might slow its progression, at least in the early stages of MS.
• Skin cancer. Some research suggests that for certain populations, vitamin D, in combination with sun exposure or calcium supplementation, might offer some protection against skin cancer.
• Type 2 diabetes. Considerable research indicates that vitamin D, often in combination with calcium, helps regulate blood sugar and may reduce the risk of type 2 diabetes.
• Vaginal infections. Bacterial vaginosis affects nearly one of every three women. Maintaining normal vitamin D levels might reduce the risk of this type of infection.
Why do we age? What is it that makes us age and grow saggy? How can we bring our youthful glow into adulthood and beyond? These are the questions that most women ask themselves. Joking, scientists and men alike ask the same questions. And you might find your answer in telomeres.
Brief Intro to Telomeres
Human cells divide at an average of 50-60 times in one lifespan. Every time they divide, the cell’s DNA has to be replicated. That way, a new chromosome can form and be used in the newly duplicated cell. However every time a cell duplicates, it comes at a cost. That is, the chromosomes get shorter and shorter. If they get short enough, the chromosomes can have their twining undone and our genetic data gets corrupted. Eventually, that cell dies.
Fortunately, chromosomes are like shoelaces with plastic caps. These plastic caps are what keep the shoelaces from getting undone. Chromosomes have their own plastic caps too. They are called telomeres. They are the extra DNA strands that a chromosome can afford to lose. They are what keep chromosomes from getting corrupt. So why are we not immortal? This is what an article from the University of Utah has to say about telomeres and division:
Yet, each time a cell divides, the telomeres get shorter. When they get too short, the cell no longer can divide and becomes inactive or “senescent” or dies. This process is associated with aging, cancer and a higher risk of death. So telomeres also have been compared with a bomb fuse.
They help to preserve genetic data when cells replicate in order to have fully functional healthy cells. RNA molecules are necessary in the process of copying DNA strands. Telomeres get shorter each time because these small RNA pieces need room on top of newly formed chromosomes.
Without telomeres, the ends of chromosomes would look like broken DNA, and the cell would try to fix something that wasn’t broken. That also would make them stop dividing and eventually die.
Telomerase, Cancer, and Aging
So is there something that keeps telomeres from disappearing? Actually there is an enzyme called telomerase. They fit on top of telomeres and are more prevalent in the younger years, however they also eventually disappear.
This is not the case for cancerous cells. Cancer cells activate the telomerase enzymes once the telomeres get dangerously short. This keeps the cancer cell’s DNA intact and allows them to multiply like mad dogs. In fact, measuring telomerase may be a new way to detect new cancer threats. If we learn how to stop telomerase from being activated, we may be able to make cancer cells experience aging just like healthy cells.
In one experiment, researchers blocked telomerase activity in human breast and prostate cancer cells growing in the laboratory, prompting the tumor cells to die. But there are risks.
Shorter telomeres are related to shorter lives. Unfortunately, there is no strong evidence yet that shows that telomerase can make cells immortal and prevent aging. There is also no strong evidence that raising telomerase levels would also trigger cancerous cells to form.
Laboratory tests have shown though that telomerase was able to keep human cells divide far beyond the average limit without becoming cancerous. If researched further, we can have a future where human cells can be mass produced for transplantation, especially in key roles such as cells that produce insulin for diabetes patients.
Lets begin, continue, finish, and be confused with the numbers. As 2013 taxes have yet to be collected, I’ll be examining the collected tax statistics for 2011. From the 2011 IRS Data Book:
Aside from selling treasury shares which collect huge amounts of interest, tax revenues are the only way in which our government gets money. So every paycheck you give money to the government in exchange for a service. Do you like the results that you’re getting?
Now that we know how much money the great tax vacuum inhales every year lets examine the federal budget spending (outlays in billions of dollars) for that same year:
As you can see, the majority of spending is divided between discretionary programs and mandatory programs. Social security, medicare, medicaid, and other programs received approximately $2 trillion dollars in government spending. Great, we’ve got around $400 billion left! Lets spend it on some cool stuff that will make us all happier.
Right away we’ve got a problem: The defense budget is allocated almost $700 billion. That’s 30% of 2011 total collected tax revenue.
…nearly all of the federal government’s investments in primary and secondary education, in transportation infrastructure, and in scientific, technological, and health care research and development. It also includes nearly all of the federal government’s law enforcement resources, as well as essentially all federal efforts to keep our air, water, food, pharmaceuticals, consumer products, workplaces, highways, airports, coasts, and borders safe. It includes veterans’ health care services and some nutritional, housing, and child care assistance to low-income families. It even includes the funding for such national treasures as the Smithsonian Institution, our national parks system, and the National Aeronautics and Space Administration, better known as NASA.
In lay speak that means: all of the neat stuff.
Next on the list comes the net interest. $230 billion dollars of interest was accrued by previous treasury bonds. In the unlikely case that you are completely unaware of debt and its practice; interest accrued is a compounding tax on borrowed money. It acts as incentive for borrowers, giving them a payout for “helping” a country in need. As the U.S. general public holds $11,855,687,948,374.48 in debt, I’ll spare you any more ironic explanations of debt.
Wait a second. Wait just one second. In 2011 the U.S. Government spent approximately $3.6 trillion. The tax revenue accounts for approximately 67% of that money spent. So, as I stated earlier, the other 32% must come from treasury shares. That means that almost a third of our 2011 spending was covered by a pseudo-credit card.
So who all helped finance our deficit? The chart to the left shows the amount of money, in billions of dollars, that the united states owes to various countries and companies.
China and Japan rake in the most with a combined $2.1 trillion. To put that into perspective that’s almost the entire collected tax revenue for 2011. An entire year of hardworking laborers would just barely be able to pay off these two debts. This is assuming that the United States spends absolutely nothing on anything else.
So, when you hear about congress and the president running around every year trying to figure out a budget, you now have a better understanding of what the heck they are actually doing. Every person has a different idea of what the United States budget should be and when there are outside interests holding gigantic stakes there is absolutely no easy way to get out of this.
The best way to fix anything is to start small. A billion dollars here a billion dollars there. It might be an idea to start turning off the white house bowling alley an hour earlier each night.
Freon represents several different chlorofluorocarbons, or CFCs, which are used in commerce and industry. The CFCs are a group of aliphatic organic compounds containing the elements carbon and fluorine, and, in many cases, other halogens (especially chlorine) and hydrogen. Freons are colorless, odorless, nonflammable, noncorrosive gases or liquids […] CFCs, or Freon, are now infamous for greatly adding to the depletion of the earth’s ozone shield.
A couple years ago, Electrolux Design Labs ran a contest for household appliance redesigns. Two of the finalists caught my eye and gave my inner hippie hope for the future, specifically, the Future Gel and Honeycomb models (not their official names, just how I will be referring to them in this article for the sake of being consistent and concise).
Utilizes a special gel-like substance that suspends and cools food once inserted.
The Bio Robot Refrigerator mounts on a wall—Dmitriev points out it can be mounted horizontally, vertically or even on the ceiling. The fridge does not have a motor or other traditional technology like most refrigerators—the gel does all the work—so, 90% of the appliance is actual usable space. To use the fridge you basically shove food into it’s biopolymer gel—which has no odor and is not sticky—and it is suspended and cooled until you need it again.
I’m not quite sure how far we are from biopolymer gel, but the idea is fascinating nonetheless.
The other design that intrigued me was Ben de la Roche’s. De la Roche was, at the time of this contest at least, an industrial design student at New Zealand’s Massey University. His design uses the honeycomb pattern found in nature to make a modularized, door-less, open-front refrigeration system which saves energy by only cooling the food that’s put in it. This is accomplished through the modular interface. A traditional fridge is essentially a box that gets really cold, so if you want things (food, flowers, a human head if you’re BBC’s Sherlock, etc) to be cold, you stick it in the box. De la Roche’s design allows the cooling mechanism to be much more targeted so that the entire infrastructure isn’t being cooled unnecessarily when all that’s in it is a case of beer and collegiate hunger. This design implements thermoacoustic refrigeration using nitrogen instead of CFCs.
Prototypes or not, I’m excited about what this kind of thinking can mean for the future. Functional, aesthetically pleasing designs that make our world cleaner and safer is what I’m all about. That and food—daylight savings time coupled with all this fridge talk has thrown me for a loop. I’m hungry.
Even more amazingly, studies all around the world have concluded with exponentially growing empirical affirmation that cannabis completely and totally cures cancer. It additionally acts as a preventative, stopping cancer from ever coming back. Don’t believe me? Continue reading, or just ask the US government; they own the patent for cannabis as a successful cure and/or treatment for a whole array of medical conditions.
So why then is cannabis labeled as a schedule 1 drug, or in laymen terms, a dangerous, highly addictive substance devoid of any medical benefit? Tobacco has absolutely no medical benefits, is proven to cause cancer, is proven to kill hundreds of thousands of people worldwide, and is one of the most physically and psychologically addictive substances on the planet. However, tobacco, like alcohol, isn’t even scheduled. Additionally, cannabis is scheduled as even more dangerous, more addictive, and less medicinally beneficial then cocaine or methamphetamine, which are labeled as schedule 2 substances. As another example of the illogical scheduling process, psilocybin mushrooms, LSD, and DMT, which have been proven to be highly effective to cure cluster headaches as well as an invaluable tool in psychotherapy, are labeled as schedule 1 drugs despite these psychedelics having little to no addiction potential. Are you starting to see how silly this is? So what gives?
Let’s walk through this one step at a time. We are going to go over the historical use and legality of cannabis, the current legal status of cannabis around the world, the effects of keeping cannabis and other drugs illegal, and finally, the miraculous medicinal properties of cannabis. Feel free to jump around, but to gain a fully comprehensive understanding of this complex issue, I highly recommend reading all of this information.
Cannabis is a natural human pastime, embedded into our epigenetic expression. It was used for centuries as a form of relaxation, as a tool for meditation during religious ceremonies, and as a way to foster creativity. Additionally, hemp is one of the oldest domesticated plants known. Hemp was used in various industries, optimizing productivity, efficiency, and waste management. Then one day, cannabis and hemp were suddenly seen as cesspools of sin originating from the pits of hell.
Both hemp and cannabis were made illegal for multiple reasons, but the most prominent reasons were due to money, ignorance, and irrational racism. All around the world cannabis and hemp were being criminalized simply by default; by tossing them in a category with substances that were highly addictive (opium, morphine, etc.). There was no consideration for each substance’s individual pros and cons, and certainly no empirical scientific basis. Anything with even the slightest amount of potential for addiction was just labeled together as a harmful/addictive substance, and that was that. The US took a similar approach.
In an attempt to make substance regulation laws more uniform, all states were encouraged to regulate cannabis in the same way, essentially handing over control to the federal level. Up until this point cannabis was still legal and available as a medicine; it was simply regulated while its recreational use was criminalized. Then along came Harry Anslinger, the future head of the Federal Bureau of Narcotics, and a nuclear bomb of lies, deceit and propaganda was dropped onto the US and the world at large.
There are 100,000 total marijuana smokers in the US, and most are Negroes, Hispanics, Filipinos, and entertainers. Their Satanic music, jazz, and swing, result from marijuana use. This marijuana causes white women to seek sexual relations with Negroes, entertainers, and any others.
…the primary reason to outlaw marijuana is its effect on the degenerate races.
Marijuana is an addictive drug which produces in its users insanity, criminality, and death.
Reefer makes darkies think they’re as good as white men.
Marihuana leads to pacifism and communist brainwashing.
You smoke a joint and you’re likely to kill your brother.
Marijuana is the most violence-causing drug in the history of mankind.
We recognize these claims as utterly ridiculous nowadays, but congress back in the day wasn’t very bright. I guess some things never change.
Anslinger and his buddies were also directly responsible for the propaganda video entitled “Reefer Madness,” depicting young men and women becoming violent, sex crazed, and downright insane after smoking cannabis. “Reefer Madness” was seen as a legitimate informational source at the time of its release and for many decades afterward. It is now shown to students as a form of retrospective humor. Anslinger used baseless scare tactics in an attempt to bolster criminalization laws in the US regarding cannabis, and even more astounding, industrial hemp, which can in no way get a person high.
What should you take out of this brief history lesson? Congress made cannabis(a great medicine) and hemp (a product that would revolutionize countless industries) illegal because of a silly, sensationalized, utterly unscientific movie shown to school children. They disregarded the claims made by experts and medical professionals. They ignored the pleas for rational thought and sensibility. They had no reason to make cannabis illegal, and still don’t. I guess that’s why times are changing so quickly!
Contemporary Legality
In the latter half of the 20th century, rational substance reform finally began to take a turn with actual long term medical/economic/political/social implications of each individual substance in mind. It became clear that the historical basis for keeping cannabis illegal is entirely political and has nothing to do with science. Just think, even main stream media and most countries around the world still refer to cannabis with a name spawned from mindless propaganda; marijuana.
People all around the world have begun to see that the war on drugs has completely failed in every way imaginable, actually leading to more drug use and significantly more violence worldwide. This is due to the fact that the war on drugs only fights the symptoms of a disease deeply ingrained into our society, and I’m not talking about drug use; I’m referring to gangs/organized drug cartels. In response to the effectiveness of incarceration on drug crimes, the Public Safety Performance Project found that:
Once incarcerated, drug dealers tend to be quickly replaced by new dealers and, as during the crack epidemic, the new recruits can be younger and more prone to violence than their predecessors. Thus while drug dealers no doubt deserve punishment, most leading researchers, and many law enforcement officials, now agree that incarcerating the foot soldiers in drug gangs, not to mention drug users, has a negligible impact on crime. Moreover, by creating job openings in drug-dealing organizations, it draws more people into criminal lifestyles and may in certain cases exacerbate crime.
More than 9.8 million people are held in penal institutions throughout the world, mostly as pre-trial detainees (remand prisoners) or as sentenced prisoners. Almost half of these are in the United States (2.29m), Russia (0.89m) or China (1.57m sentenced prisoners).
Taxpayers spent about $68.7 billion in 2008 to feed, clothe, and provide medical care to prisoners in county jails, state and federal prisons and facilities housing legal and illegal aliens facing possible deportation. From 1982 to 2002, state and federal spending on corrections, not adjusted for inflation, rose by 423%, from $40 to $209 per U.S. resident. Corrections spending, as a share of state budgets, rose faster than health care, education, and natural resources spending from 1986 to 2001. The average cost of housing a prisoner for a year was about $24,000 in 2005, though rates vary from state to state.
That incredible spending increase from 1982 to 2002 coincides precisely with the increase of drug arrests due to the failed ‘war on drugs.’ This is an especially important point to consider since drug offenses are almost entirely non-violent, and rehabilitation costs significantly less for tax payers.
Treatment delivered in the community is one of the most cost-effective ways to prevent such crimes and costs approximately $20,000 less than incarceration per person per year. A study by the Washington State Institute for Public Policy found that every dollar spent on drug treatment in the community yields over $18in cost savings related to crime. In comparison, prisons only yield $.37 in public safety benefit per dollar spent. Releasing people to supervision and making treatment accessible is an effective way of reducing problematic drug use, reducing crime associated with drug use and reducing the number of people in prison.
… the benefit to counties where private prisons are built and operated can be quite scant — some receive less than $2 per prisoner per day from the private prison operator…the federal government agreed to pay CCA [one of the largest private prison firms] almost $90 per day for each detained immigrant at a San Diego facility.
Today, private companies imprison roughly 130,000 prisoners and, according to one group, 16,000 civil immigration detainees in the United States at any given time. As states send more and more people to prison, they funnel ever greater amounts of taxpayer money to private prison operators. By 2010, annual revenues of the two top private prison companies alone stood at nearly $3 billion.
Many political leaders, heads of agencies, and medical professionals are also pointing out how ridiculous it is that extremely addictive, highly toxic substances like tobacco and alcohol go unchecked while a harmless substance like cannabis remains globally demonized. Ask yourself, if alcohol were discovered today would it even be legal? In the UK, the chief drug adviser Prof. David Nutt was fired for pointing out the dangers of alcohol and nicotine and further explaining that they are for more dangerous and harmful than cannabis. Another UK drug adviser recently resigned from his job in protest of David Nutt’s silencing.
It does not make sense from a prioritization point of view for us to focus on recreational drug users in a state that has already said that under state law that’s legal.
President Obama’s response was typical of all political speech; evasive and vague. While tokers all around the country take bets on the fed’s actions, there is a significant amount of pressure on the white house to legalize cannabis at the federal level. Various bills are being presented in Congress to repeal cannabis laws and broaden economic opportunities. Although there are steps you can take, like signing this petition to give states the right to regulate cannabis however they want, decisions and movement at the federal level remain slow and stagnant as usual.
So, countries all around the world along with a growing number of US states are decriminalizing cannabis for personal use, legalizing cannabis as a medicine (or entirely legalizing it), and the US government owns a patent on medicinal cannabis as well as supplies certain patients with medical cannabis for life. What’s all the hype over cannabis? It just so happens that cannabis is a wonder-drug; a miracle for millions; potentially billions.
The Endocannabinoid System
Cannabis is one of the most highly effective medicinal substances in the world. It has the power to treat and/or cure a countless number of illnesses and syndromes, including a whole array of different types of cancer. But how can a single substance have such an extraordinary effect on our biology? It all begins with the endocannabinoid system.
Because the discovery of the endocannabinoid system is relatively new, and despite there being over 12,000 scientific articles concerning the endocannabinoid system, there are still gaps in our understanding. There is still a significant amount of research that needs to be done, and educating people on the actual science of cannabis’ activity in the body will help to clear the smoke of ignorance and closed mindedness. Once people embrace the current research that is taking place, further research into more specific and particular roles of the endocannabanoid system will take off at lightning speed. What we do know is the following:
Endocannabinoids are the substances our bodies naturally make to stimulate these receptors. The two most well understood of these molecules are called anandamide and 2-arachidonoylglycerol (2-AG). They are synthesized on-demand from cell membrane arachidonic acid derivatives, have a local effect and short half-life before being degraded by the enzymes fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase (MAGL).
Phytocannabinoids are plant substances that stimulate cannabinoid receptors. Delta-9-tetrahydrocannabinol, or THC, is the most psychoactive and certainly the most famous of these substances, but other cannabinoids such as cannabidiol (CBD) and cannabinol (CBN) are gaining the interest of researchers due to a variety of healing properties. Most phytocannabinoids have been isolated from cannabis sativa, but other medical herbs, such as echinacea purpura, have been found to contain non-psychoactive cannabinoids as well.
The information above focuses on the two most well known endocannabinoids in the body, as well as the most well known cannabinoids in cannabis, but there are far more. Cannabinoids are split into three categories:
It is through the encocannabinoid system that cannabis is able to perform its magic. Cannabis has the ability to treat and/or cure a constantly growing list of illnesses, including cancer. Dependent on the individual and the type of cannabinoid used, most types of cancer have been observed responding positively to the introduction of cannabis in the system, including cancer found in the breast, prostate, lung, thyroid, colon, skin, pituitary gland, ovary, pancreas, as well asmelanoma, leukemiaandmore! The cannabinoids in cannabis act through the body’s natural endocannabinoid system to cure and/or treat cancer in several ways, the most prominent and well researched being:
One of the greatest benefits of cannabis as medicine is that it stimulates and acts in harmony with a system that is already present throughout the body. Instead of prescribing five or more different, highly addictive pills to treat various symptoms, and additional pills to treat the endless side effects (often worse than the illness itself) of all the pills, doctors are able to use cannabis and the cannabanoids within it, as a single, natural medicinal source without any physical addiction potential and little to no harmful side effects. Plus, don’t forget, it is impossible to overdose on.
Cannabis Cures Everything Else
Along with treating various forms of cancer, cannabis can be used to treat a constantly growing list of other diseases and syndromes as well. It may even slow the aging process. Additionally, the cannabinoids found in cannabis are exceptional anti-oxidants and neuroprotectants. It is such a remarkable substance that it is able to treat seemingly opposite illnesses simultaneously, like obesity and eating disorders/malnutrition. Again, the key is the activation and involvement with the endocannabinoid system. Cannabis has shown results ranging from promising potential to revolutionary effectiveness in curing and/or treating:
(*Note: each of these words link to an individual study)
It is because the cannabinoids in cannabis are so influential on the endocannabinoid system, a system that spans every part of our body, that they are able to have such an effective, overarching, revolutionarily positive effect. Keep in mind that the above is what researchers have found with limited funds, little time, and immense legal obstacles. The golden age of cannabis research hasn’t even started yet.
What the Critics Have to Say
(And Why They’re Wrong…)
On the flip side, critics are quick to point out the consistently noted dangers of cannabis ingestion. These are the same arguments that have been used for decades. They remain aggressively debated without compromise, despite decades of rational evidence suggesting falsity and fallacy. The seemingly valid concerns regarding cannabis use that top the critics’ list are: the gateway drug theory, short-term memory loss, psychosis, decreased intelligence, harm from cannabis smoke, depression, an elevated heart rate, and worries over driving while high. Let’s allow science and logic to save the day, shall we?
Gateway Drug
Many critics of cannabis use claim that cannabis is a gateway to harder and more persistent drug use. They are implying that if a person uses cannabis, recreationally or medically, they are more likely to use dangerous drugs like cocaine (again, ironically listed as a schedule 2 drug) or heroin. Although multiple studies have found that cannabis users are more likely than non-users to engage in the use of more ‘hardcore’ substances (meaning higher addiction potential and/or more biologically detrimental), there are endless holes in this argument.
Much of their [US drug-policy leaders] rhetoric about marijuana being a ‘gateway drug’ is simply wrong. After decades of looking, scientists still have no evidence that marijuana causes people to use harder drugs. If there is any true ‘gateway drug,’ it’s tobacco.
Alcohol and tobacco are more accessible and far more likely to be used by teens, consequently making those substances more likely to lead to further drug use. As stated by Elders, they are the true gateway drugs. In one of the most highly credible and sourced assessments on the science of drug use, the Institute of Medicine stated that:
In fact, most drug users do not begin their drug use with marijuana–they begin with alcohol and nicotine, usually when they are too young to do so legally…
There is no evidence that marijuana serves as a stepping stone on the basis of its particular physiological effect.
Starting to see the trend here? Alcohol and tobacco are far more dangerous and addictive than cannabis. If the gateway drug theory did have any legitimacy, it would have to be applied to alcohol and nicotine, two completely legal substances, before it could be attributed to any other substance.
The best analogy I’ve ever encountered for the ridiculousness of the gateway drug theory comes from Lynn Zimmer, PhD, Professor Emeritus at Queens College at the City University of New York:
In the end, the gateway theory is not a theory at all. It is a description of the typical sequence in which multiple-drug users initiate the use of high-prevalence and low-prevalence drugs.
A similar statistical relationship exists between other kinds of common and uncommon related activities. For example, most people who ride a motorcycle (a fairly rare activity) have ridden a bicycle (a fairly common activity). Indeed, the prevalence of motorcycle riding among people who have never ridden a bicycle is probably extremely low. However, bicycle riding does not cause motorcycle riding, and increases in the former will not lead automatically to increases in the latter.
Nor will increases in marijuana use lead automatically to increases in the use of cocaine or heroin.
If we overly criminalize behaviors like marijuana use among teens, this could interfere with opportunities for education and employment later on, which, in turn, could be creating more drug use.
The gateway drug theory is weak and unfounded. It is in fact not a credible theory at all. It has no place in the realm of science.
Decreased Intelligence
It is a propaganda technique that we have been hearing for nearly the entire 20th century and it continues into the 21st century; cannabis makes you stupid, a loser, a burnout.
While there is clear evidence that cannabis, like other substances, alters perception and brain function, there is no evidence that cannabis alters brain function in a purely negative way. Additionally, there is absolutely zero evidence that the biological effects of cannabis are permanent. On the contrary, science tells us that all of the consistently noted negative biological aspects of cannabis are entirely temporary.
According to Igor Grant, MD, Executive Vice Chairman at the University of California, San Diego Department of Psychiatry:
Smoking marijuana will certainly affect perception, but it does not cause permanent brain damage. ‘The findings were kind of a surprise. One might have expected to see more impairment of higher mental function. Other illegal drugs, or even alcohol, can cause brain damage…
If we barely find this tiny effect in long-term heavy users of cannabis, then we are unlikely to see deleterious side effects in indivduals who receive cannabis for a short time in a medical setting…
If it turned out that new studies find that cannabis is helpful in treating some medical conditions, this enables us to see a marginal level of safety.
Government experts now admit that pot doesn’t kill brain cells.
This myth came from a handful of animal experiments in which structural changes (not actual cell death, as is often alleged) were observed in brain cells of animals exposed to high doses of pot. Many critics still cite the notorious monkey studies of Dr. Robert G. Heath, which purported to find brain damage in three monkeys that had been heavily dosed with cannabis. This work was never replicated and has since been discredited by a pair of better controlled, much larger monkey studies, one by Dr. William Slikker of the National Center for Toxicological Research [William Slikker et al., ‘Chronic Marijuana Smoke Exposure in the Rhesus Monkey,’ Fundamental and Applied Toxicology 17: 321-32 (1991)] and the other by Charles Rebert and Gordon Pryor of SRI International [Charles Rebert & Gordon Pryor – ‘Chronic Inhalation of Marijuana Smoke and Brain Electrophysiology of Rhesus Monkeys,’International Journal of Psychophysiology V 14, p.144, 1993].
Neither found any evidence of physical alteration in the brains of monkeys exposed to daily doses of pot for up to a year.
The surprising truth is that cannabis actually promotes the creation of new neurons in hippocampal regions of the brain, the part of the brain most responsible for memory. Xia Zhang, an expert at the Neuropsychiatry Research Unit, Department of Psychiatry, at the University of Saskatchewan in Canada along with other medical researchers, points out that cannabis is the only illicit drug ever found to promote the creation of brain cells:
We show that 1 month after chronic HU210 [high-potency cannabinoid] treatment, rats display increased newborn neurons [brain cell growth] in the hippocampal dentate gyrus [a portion of the brain] and significantly reduced measures of anxiety- and depression-like behavior.Thus, cannabinoids appear to be the only illicit drug whose capacity to produce increased hippocampal newborn neurons is positively correlated with its anxiolytic- [anxiety reducing] and antidepressant-like effects.
College students who smoke cannabis demonstrate comparable or even higher grades than their cannabis abstinent classmates, and are more likely to pursue a graduate degree.
The short answer is yes, cannabis alters your mind and body, like any other substance in the world, but it does not make you stupid (certainly you’re not going to claim any of these highly successful cannabis-users are stupid), and all of the physiological and psychological effects are temporary.
Critics of cannabis use argue that memory loss, especially short-term memory loss, occurs more prominently in cannabis smokers. They also claim that it is a permanent effect. All of these claims are either exaggerated or wrong. We’ve already discussed how all the effects of cannabis ingestion are completely temporary; the same applies to memory.
To begin, it is true that cannabis has a noticeable effect on short-term memory as well as working memory, while the user is under the influence. Cannabis affects working memory through the mechanisms stated above, by encouraging neurogensis, or the creation of neurons, in the hippocampus region of the brain. Although this has a positive effect on memory overall, it disrupts short-term memory while the user is ‘high’ by creating ‘noise’ in the hippocampus. These effects are detectable at least 7 days after heavy cannabis use,
but appear reversible and related to recent cannabis exposure rather than irreversible and related to cumulative lifetime use.
Furthermore, after extensively studying cannabis use, lead researcher and Harvard professor Harrison Pope came to the conclusion that:
From neuropsychological tests chronic cannabis users showed difficulties, with verbal memory in particular, for ‘at least a week or two’ after they stopped smoking.Within 28 days, memory problems vanished and the subjects ‘were no longer distinguishable from the comparison group.’
These tests affirm that the physio/psychological effects of cannabis are temporary and reversible.
As for the seriousness of the temporary effects on short-term memory, studies have found that the effect is negligible. Researchers from the University of California, San Diego School of Medicine headed by Dr. Igor Grant analyzed data from 15 previously published controlled studies involving 704 long-term cannabis users and 484 nonusers and found that:
long-term cannabis use [is] only marginally harmful on the memory and learning. Other functions such as reaction time, attention, language, reasoning ability, perceptual and motor skills [are] unaffected. The observed effects on memory and learning, [show] long-term cannabis use [causes] ‘selective memory defects’, but that the impact [is] ‘of a very small magnitude.’
In fact, rather than having deleterious effects on memory, Ohio State University scientists have shown that
Research supports this claim as past studies have revealed that cannabinoid receptors stimulated by cannabinoids in cannabis act as an anti-inflammatory agent and serve to improve memory in old rats.
Surprisingly, recent research into the activity of the hippocampus suggests that the key to a good memory is forgetting. Think of the brain as a computer with enormous hard drive space. Despite this incredible amount of storage, it is still finite. The more memories our brains create, the harder it is for our working memory to properly remember and recall. In this way, forgetting a few things actually isn’t a bad thing. It is in fact highly beneficial overall.
Another important point is that different cannabinoids found in cannabis affect memory centers in the brain in remarkably different ways. Through further legalization, scientists will have the freedom to perform more extensive research, while growers will have the opportunity to create strains of cannabis that have an even more minimal effect on the memory centers of the brain.
These studies reveal that in the short run, short-term and working memory are disrupted by the ingestion of cannabis by creating new neurons in the memory centers of the brain. These additional neurons disrupt working memory by acting as additional ‘noise’ to the active, recalling mind. These short-term memory lapses are completely temporary though, and in the long run the brain is actually left with additional neurons and a more expansive memory center. To use the analogy of a computer again, think of heavy-cannabis ingestion as a temporary lapse in primary memory functionality for the sake of upgrading the storage capabilities of secondary memory.
Elevated Heart Rate
It is true that many cannabis users describe symptoms of panic and consequently an elevated heart rate, especially during their first time trying cannabis. What still remains debated is whether cannabis itself biologically causes heart rate to increase.
The most well known study done on the correlation between cannabis and heart rate, and subsequently the only truly credible and widely used study, is one performed by a man named Dr. Murray A. Mittleman. Mittleman’s study focused on:
information on cannabis use from 3,882 middle-aged and elderly patients who had suffered heart attacks. A total of 124 patients were identified as current users, including 37 who reported smoking the drug up to 24 hours before their attack, and nine who had used it within an hour of experiencing symptoms.
Mittleman’s conclusion was that the first hour after taking cannabis heart attack risk is 4.8 times higher than during periods of non-use. In the second hour, the risk drops to 1.7 times higher. According to Mittleman this was the first study to document that smoking cannabis could trigger a heart attack, but that the trigger mechanism remained unknown. So what’s the issue with this constantly cited study?
Besides the fact that any type of smoke entering the lungs produces the same effect (it is not necessary and not medicinally optimal to smoke cannabis, a subject that is covered later in this report), Dr. Lester Grinspoon, who is one of the world’s foremost cannabis researchers as well as Associate Professor Emeritus of Psychiatry at Harvard Medical School and a former senior psychiatrist at the Massachusetts Mental Health Center in Boston for 40 years, explains why this study should be dismissed. Dr. Grinspoon tells an interviewer, in response to Mittleman’s study:
..let me say that since 1967 there have been numerous reports and studies, each of which the American media has blown out of all proportion, stating one or another supposed ill effect of marijuana use. I can list them, if you’d like. ‘Increase in the size of the ventricles, decrease in testosterone, destruction of chromosomes.’ All were front-page stories, none of them have ever been replicated. In other words, they didn’t pan out scientifically. Of course, the studies that contradicted them ended up on page 31 or thereabouts, if they got mentioned at all… I would point out that out of 3,882 patients, we’re talking about 9 who used marijuana within an hour of the onset of a heart attack. That’s around 0.2%. By sheer mathematics, given that people sleep eight hours per day or so, we can deduce that 6.7% of those patients emptied their bowels within an hour of onset. It’s incredible to me that the numbers here could be said to constitute a significant risk factor.
So, as is typical of the main stream media, a report was utterly sensationalized and relatively negligible data was heralded as proven truth. Dr. Grinspoon elaborates on the shortcomings of the study by reminding the interviewer that:
[Mittleman] put that increase [in heart rate] at 40 beats per minute. In truth, that number is closer to 20 beats per minute, which is probably consistent with running up the stairs in one’s house...I blame the media far more than I do Dr. Middleman. I read his abstract, and in its conclusion he cautioned against making too much of the data…in 1997, Kaiser Permanente did a large-scale study which included more than 65,000 admitted marijuana users, and they could not demonstrate any impact of marijuana use on mortality. If marijuana use really was a significant risk factor for heart attack, it is hard to believe that it didn’t turn up there. Again, I’m not saying that there is absolutely no risk demonstrated here. But given the history of the research since 1967, I’d be surprised if these findings don’t go down the same chute as all of the other front-page scare stories.
It’s really not that hard to believe. We have seen the same baseless scare tactics take place 20 years ago, 40 years ago, 60 years ago, 100 years, and more!
With regards to actual significant scientific data, cannabis has in fact been shown (as stated in the ‘Cannabis Cures Everything’ section of this report) to treat and protect the heart, as well as help prevent heart disease through the interaction with the endocannabinoid system of the heart and surrounding regions of the body. It is consequently a likely tool for fighting and preventing obesity (along with hemp seeds). The science is still emerging, but what little research exists strongly suggests that cannabis will serve an extremely positive role in keeping the heart healthy in the future.
The single study that is consistently used to argue that cannabis poses a danger to cardiovascular health is far from significant and only became prominent through sensationalized media. Repeat studies suggest the cannabinoids found in cannabis play a pivotal role in cardiovascular health and the prevention of heart disease.
Psychosis
An historically major issue concerning cannabis is the worry that it may induce schizophrenic symptoms or intensify various forms of latent schizophrenia. The subjective experience of ingesting cannabis is highly personal and varies greatly among users around the world. Common experiences include:
Greater enjoyment of food taste and aroma
blogs.sfweekly.com
An enhanced enjoyment of music
A greater enjoyment of comedy and humor
Distortions in perception of time and space
Short-term memory loss
Improved long-term memory recall
Creative thinking
New perspectives
Increased libido
Elevated mood
Heightened sensitivity to external stimuli
Relaxation
At extremely high doses common experiences include:
Altered body image
Auditory/visual illusions
Hallucinations (extremely rare)
Mild dissociation of mind and body
Panic attacks
Paranoia
While the vast majority of the effects of cannabis are viewed as positive, panic attacks and paranoia are obviously unwanted. Between 20 and 30 percent of recreational users experience intense anxiety and/or panic attacks after smoking cannabis.
While these symptoms usually occur due to thoughts of legal ramification for ingesting cannabis, exaggerated worry over a thought process, or general anxiousness over trying something new, it has been reported that the symptoms can happen spontaneously as well. It is possible and plausible that these symptoms could lead to greater and more persistent symptoms of psychosis. However, there are multiple aspects of the psychosis worry that needs to be discussed.
First, through our increasing knowledge of cannabinoids and the role they play on the endocannabinoid system, researchers have discovered that certain cannabinoids have a marginally stronger effect than others with regards to producing hallucinations delusions, and subjective psychological stress.
While the THC (the most psychoactive cannabinoid found in cannabis) offers incredible physio/psychological health benefits, it has been linked to being the sole culprit of producing more schizophrenia-like symptoms.
When comparing multiple subjects under the influence of only THC, a mixture of THC and CBD (cannabidiol), and no cannabinoids, researchers found that only THC produced subjectively negative psychological effects. The subjects with no additional cannabinoids in their system and the subjects with the mixture of THC and CBD both experienced a nearly identical psychological effect. The only major difference was that the subjects who had ingested the mixture reported less anhedonia (unable to experience pleasure) then the other two groups. The researchers concluded that if anything, their research highlighted
the importance of distinguishing between different strains of cannabis.
Once we break cannabis down into its component cannabinoids it is easy to see why users describe such incredibly varied experiences. Cannabidiol is extremely effective in treating and preventing symptoms of schizophrenia, as research continues to suggest. Many researchers believe that cannabis legalization will herald a revolution in the treatment of various psychological disorders, including schizophrenia. According to a 2005 double-blind study analyzing the antipsychotic effects of cannabidiol, researchers found that:
cannabidiol treatment was accompanied by a significant increase in serum anandamide levels, which was significantly associated with clinical improvement. The results suggest that inhibition of anandamide deactivation may contribute to the antipsychotic effects of cannabidiol potentially representing a completely new mechanism in the treatment of schizophrenia.
Other studies on the topic affirm that many subjects report
A group of Dutch scientists say that there is no proof that cannabis induces schizophrenia. These findings will be embarrassing for the Dutch government, which has been bearing down on Marijuana Coffee Shops saying the drug induces schizophrenia.
The truth is that much of the research done thus far has been skewed and largely unscientific. Under proper guidance, and using the correct strains, researchers all around the world agree that cannabis is a wonderfully effective psychotropic medication. Researchers discussed the consistently shown promise and proof of cannabis as an effective psychotropic medication in the British Journal of Psychiatry:
I considered Arseneault et al‘s (2004) search for evidence of the association between cannabis and psychosis as quite skewed. They did not explore the evidence regarding positive, therapeutic or beneficial psychoactive effects of cannabis in mental health in the context of appropriate, rational and clinical usage…Signalling, mostly inhibitory, suggests a role for cannabinoids as therapeutic agents in central nervous system disease where inhibition of neurotransmitter release would be beneficial. Evidence suggests that cannabinoids inhibit the neurotransmitter glutamate, counteract oxidative damage to dopaminergic neurons and may be potent neuroprotective agents (Croxford, 2003)…knowing [cannabis’] potent neuroprotective function, its potential role in psychiatric practice should not be discarded lightly.
The most important thing to remember is that symptoms of schizophrenia generally (nearly always) precede cannabis use. Schizophrenia and general psychosis have far more to do with genetic make up than anything else (refer to the graph).
Research regarding the connection between cannabis and psychosis, especially symptoms of schizophrenia, remains historically lacking and skewed with regards to component cannabinoids in cannabis. Cannabis produces highly varied subjective experiences, and research has revealed that each cannabinoid within cannabis has a markedly different effect on individuals. Multiple recent studies have shown that cannabis, specifically the cannabinoid CBD, is a highly effective agent in treating schizophrenia and other psychological disorders. Most importantly, symptoms of schizophrenia precede cannabis use in the vast majority of cases. There is currently no clear evidence that cannabis is directly responsible for causing psychosis and schizophrenic symptoms in users.
Depression
This is one of the most commonly used arguments against the use of cannabis as a form of medicine or recreation. Like the psychosis argument debunked above, the depression argument is always portrayed in a skewed and exaggerated fashion. The most important thing to remember as we discuss this is that correlation does not imply causation.
forum.grasscity.com
It is well known that many already depressed individuals (ranging from mild to incapacitating depression) use cannabis as a form of self-medication. This often takes place after finding no success with taking a whole slew of expensive, addictive, and biologically destructive prescription drugs handed out by the oh so helpful DSM devotees.
Over 4400 adult internet users [who] completed The Center for Epidemiologic Studies Depression scale and measures of marijuana use. We employed an internet survey in an effort to recruit the most depressed and marijuana involved participants, including those who might prove unwilling to travel to the laboratory or discuss drug use on the phone or in person. We compared those who consumed marijuana daily, once a week or less, or never in their lives. Despite comparable ranges of scores on all depression subscales, those who used once per week or less had less depressed mood, more positive affect, and fewer somatic complaints than non-users. Daily users reported less depressed mood and more positive affect than non-users. The three groups did not differ on interpersonal symptoms.
Cannabis users, whether they ingested the substance less than once a week or every day, reported far less depressive symptoms and far more happiness and satisfaction than non-users. The study goes on to say that:
The media continues to report links between marijuana and depression. In a recent review, Degenhardt, Hall, and Lynskey (2003) identified a modest relationship only among problematic users. Many studies show no link between cannabis and depression despite appropriate statistical power, measurement, and design (Fergusson & Horwood, 1997; Fergusson, Lynskey, & Horwood, 1996; Green & Ritter, 2000; Kouri, Pope, Yurgelun-Todd, & Gruber, 1995; McGee, Williams, Poulton, & Moffitt, 2000; Musty & Kaback, 1995; Rowe, Fleming, Barry, Manwell, & Kropp, 1995). One neglected source of depression among marijuana users may stem from medical use. Separate analyses for medical vs. recreational users demonstrated that medical users reported more depressed mood and more somatic complaints than recreational users, suggesting that medical conditions clearly contribute to depression scores and should be considered in studies of marijuana and depression. The data suggests that adults apparently do not increase their risk for depression by using marijuana.
Just like we discussed in all of the other arguments, the public only sees what the media picks and chooses to show, which is usually negligible data that has been exaggerated and skewed to fit their hype. The previous study also brought up an excellent point that has never been discussed before: are the results of studies concerning cannabis and depression that get aired by main stream media corrupted by reports of depression that originate from medical suffering? The use of cannabis is so wide spread around the world, especially in the US, that it should not be discounted.
After adjusting for differences in baseline risk factors of marijuana use and depression, past-year marijuana use does not significantly predict later development of depression.
Finally, in a longitudinal study completed in 2009 regarding cannabis and suicide,researchers found that:
Although there was a strong association between cannabis use and suicide, this was explained by markers of psychological and behavioural problems. These results suggest that cannabis use is unlikely to have a strong effect on risk of completed suicide, either directly or as a consequence of mental health problems secondary to its use.
The depression argument is false in many of the same ways as the psychosis argument. In the vast majority of cases depressive behavior precedes cannabis use. Additionally, in most cases where cannabis is used to self-treat depression it is found to be successful. Cannabis is a clear biological antidepressant and exhibits incredible therapeutic properties. Depression is highly subjective and everyone experiences it differently. The truth is that in multiple studies both light and heavy cannabis users report far less depressive symptoms than non-users. There is no evidence whatsoever that cannabis use predicts or causes depression. Many depressed people use cannabis and report positive results far more often than people using contemporarily prescribed prescription medication.
lfp-blog.com
Driving While Stoned
(*Note: this report does not advocate driving while under the effects of any substance, including cannabis. The aim of this section is to view the credible findings on how cannabis affects drivers.)
cannabis impairs driving behavior. However, this impairment is mediated in that subjects under cannabis treatment appear to perceive that they are indeed impaired. Where they can compensate, they do.
Despite biological theories for how cannabis might potentially affect a driver, experiments using driving simulations in the lab find that:
drivers who drank alcohol overestimated their performance quality whereas those who smoked marijuana underestimated it. Perhaps as a consequence, the former invested no special effort for accomplishing the task whereas the latter did, and successfully. This evidence strongly suggests that alcohol encourages risky driving whereas THC encourages greater caution, at least in experiments.
The [findings] contrast with results from many laboratory tests, reviewed by Moskowitz (1985), which show that even low doses of THC impair skills deemed to be important for driving, such as perception, coordination, tracking and vigilance. The present studies also demonstrated that marijuana can have greater effects in laboratory than driving tests. The last study, for example showed a highly significant effect of THC on hand unsteadiness but not on driving in urban traffic.
It is apparent that despite multiple laboratory studies displaying favorable results, real world driving tests are even more positive. When we actually test the effects of cannabis on drivers in the real world, we see very little safety issues, if any at all.
Drivers under the influence of cannabis, unlike alcohol, realize they are under the effects of a substance and successfully compensate for their altered state of mind by driving slower and by giving themselves more space between other vehicles. One of the first actual road tests with cannabis studies drivers in the lab, on the highway, and in congested urban areas. The results affirmed that as far as cannabis’ effect on actual driving performance:
Driving quality as rated by the subjects contrasted with observer ratings. Alcohol impaired driving performance according to the driving instructor but subjects did not perceive it; marijuana did not impair driving performance but the subjects themselves perceived their driving performance as such….Thus there was evidence that subjects in the marijuana group were not only aware of their intoxicated condition but were also attempting to compensate for it…drivers become overconfident after drinking alcohol…and more cautious and self critical after consuming low THC doses by smoking marijuana.
Drivers under the effects of cannabis pay more attention to the road; drive more slowly, and leaving themselves more room between other cars.
The truth is that alcohol is a far more serious problem than cannabis when it comes to driving. Studies performed from 1982 to 1998 demonstrate time and time again that alcohol is significantly more dangerous than cannabis on the road. Alcohol use is also far more prevalent in crash statistics.
Blood and/or urine from fatally injured drivers in Washington State were collected and tested for the presence of drugs and alcohol. Drug and/or alcohol use was a factor in 52% of all fatalities. Among single vehicle accidents, alcohol use was a factor in 61% of cases versus 30% for multiple vehicle accidents. Drugs most commonly encountered were marijuana (11%), cocaine (3%), amphetamines (2%), together with a variety of depressant prescription medications.
The study even found that it was far less likely to find alcohol in a person’s system in the presence of cannabis, implying that cannabis use lessened the prevalence of alcohol use on the road:
Trends noted included an association of depressant use with higher blood alcohol levels, while marijuana use was associated with lower blood alcohol levels.
With regards to comparisons between cannabis and illicit substances overall, Accident Analysis & Prevention, a peer-reviewed journal, reported in its July 2004 article titled “Psychoactive Substance Use and the Risk of Motor Vehicle Accidents,” by K.L.L. Movig, et al.:
The objective of this study was to estimate the association between psychoactive drug use and motor vehicle accidents requiring hospitalization.
The risk for road trauma was increased for single use of benzodiazepines and alcohol…High relative risks were estimated for drivers using combinations of drugs and those using a combination of drugs and alcohol. Increased risks, although not statistically significant, were assessed for drivers using amphetamines… No increased risk for road trauma was found for drivers exposed to cannabis.
The largest study ever done linking road accidents with drugs and alcohol has found drivers with cannabis in their blood were no more at risk than those who were drug-free. In fact, the findings by a pharmacology team from the University of Adelaide and Transport SA showed drivers who had smoked marijuana were marginally less likely to have an accident than those who were drug-free. A study spokesman, Dr Jason White, said the difference was not great enough to be statistically significant but could be explained by anecdotal evidence that marijuana smokers were more cautious and drove more slowly because of altered time perception. The study of 2,500 accidents, which matched the blood alcohol levels of injured drivers with details from police reports, found drug-free drivers caused the accidents in 53.5 per cent of cases. Injured drivers with a blood-alcohol concentration of more than 0.05 per cent were culpable in nearly 90 per cent of accidents they were involved in. Drivers with cannabis in their blood were less likely to cause an accident, with a culpability rate of 50.6 per cent. The study has policy implications for those who argue drug detection should be a new focus for road safety. Dr White said the study showed the importance of concentrating efforts on alcohol rather than other drugs.
The BBC and CNN both filmed their own research on the actual effects of cannabis on driving ability. The BBC study focused on a single driver and found that he actually drove better while ‘high’; driving more cautiously and paying more attention to the driving test. The CNN study was a bit more extensive and controlled.
The study, conducted in Washington where recreational cannabis use is legal, focused on 3 volunteers who drove under the effects of different amounts of cannabis. They drove alongside a driving instructor with drug recognition experts (police officers with specific drug recognition training) watching them from outside the vehicle. The volunteers included a heavy daily user, a weekend user, and an occasional user. Even at 7x the legal limit of driving under the influence, 5x the legal limit, and 4x the legal limit respectively, all of the volunteers passed their driving tests, received positive reviews from the driving instructor, and would not have been pulled over by the drug recognition experts.
It’s just safer to drive under the influence of marijuana than it is drunk….Drunk drivers take more risk, they tend to go faster. They don’t realize how impaired they are. People who are under the influence of marijuana drive slower, they don’t take as many risks.
From a theoretical point of view it makes sense that people would be concerned over potential risks of ‘driving while stoned.’ However, the research speaks for itself. Laboratory and real world test results have confirmed time and time again that cannabis does not have a detrimental effect on driving ability. People under the effects of cannabis, unlike alcohol, realize their altered state of mind and compensate successfully for it. In most instances cannabis users drive more safely; driving slower, paying more attention to the road, and remaining more cautious and vigilant. Cannabis does not pose any serious danger to drivers or anyone else on the road.
atheistfoundation.org.au
Cannabis Smoke and Lung Damage
patients4medicalmarijuana.wordpress.com
There are endless reports that claim cannabis harms the lungs and bronchial airways, as well as increasing the risk of lung cancer. What you’ll quickly notice though is that the studies these reports are quoting from are completely theoretical studies based on comparisons with cigarette smoke, as opposed to actual findings from research. Additionally, they only focus on one mode of cannabis ingestion, one that destroys many of the medical benefits of cannabis; smoking.
It is true that there are over 50 potentially carcinogenic substances found in cannabis. Additionally, because smoked cannabis is not completely dry and is smoked without a filter, there is roughly 4 times more tar than the amount found in cigarettes. One can see why studies would speculate that cannabis may increase the risk of lung cancer. As usual, when you look at the actual science, the opposite is true.
First of all, there is currently not a single known case of cancer originating from the ingestion of cannabis. As stated numerous times in this report, there has never been a death that cannabis was directly responsible for.
A study in 2005, the largest ever conducted of its kind, left Donald Tashkin, a pulmonologist at UCLA‘s David Geffin School of Medicine, scratching his head. Tashkin and his research team had hypothesized an association between cannabis and lung cancer, but even after 30 years of observing thousands of subjects they were unable to find a connection between cannabis and lung cancer.
We hypothesized that there would be a positive association between marijuana use and lung cancer, and that the association would be more positive with heavier use. We expected that we would find that a history of heavy marijuana use – more than 500 to 1,000 uses – would increase the risk of cancer from several years to decades after exposure to marijuana. What we found instead was no association at all, and even a suggestion of some protective effect.
kushsmoke.com
The heaviest users in Tashkin’s study smoked more than 60 joint-years worth of marijuana, or more than 22,000 joints in their lifetime. Moderately heavy users smoked between 11,000 and 22,000 joints.
That’s an enormous amount of marijuana [however] in no category was there any increased risk, nor was there any suggestion that smoking more led to a higher odds ratio. There was no dose-response, not even a suggestion of a dose response, and in all types of cancer except one, oral cancer, the odds ratios were less than one. This is the largest case-control study ever done, and everyone had to fill out a very extensive questionnaire about marijuana use. Bias can creep into any research, but we controlled for as many confounding factors as we could, and so I believe these results have real meaning.
That being said, Dr. Tashkin wisely notes:
It’s never a good idea to take anything into your lungs, including marijuana smoke.
Smoke does not belong in your lungs, and just as this report does not advocate driving while under the effects of cannabis, it equally does not recommend smoking cannabis. What this report does suggest is using a vaporizer, cooking the cannabis into food, or making a cannabis oil. All of these methods make this entire argument irrelevant as they do not involve any form of smoke.
The media has bombarded the public with seeming ‘proof’ that cannabis leads to lung cancer. The truth is that all of this ‘proof’ has been entirely speculative. Despite cannabis smoke containing carcinogens and up to 4 times more tar than the amount found in cigarettes, long term studies confirm that there is no increased risk of lung cancer from smoking cannabis. On the contrary, the cannabinoids found in THC work to fight against cancer and even protect healthy cells. Most importantly, because cannabis can be ingested in many ways that don’t involve smoke, this entire argument is irrelevant.
Cannabis Oil: Run From the Cure
The most medicinally beneficial way to ingest cannabis is by making a high potency cannabis oil. It should be clear now from this report that cannabis is far more effective than conventional medicine for a near-endless variety of ailments. This is especially true for cancer.
The point is, no matter what type of conventional medicine you use, your chances of survival are bleak, and the side effects are horrendous. On the other hand, there is a medicine available that has been proven to completely cure cancer in the majority of cases, as well as having little to no adverse side effects. Additionally, it is as non-toxic as a substance can get, and is impossible to overdose on. Plus, it focuses on treating the side effects of cancer along with the cancer itself. At this point, you recognize that I’m referring to cannabis, but in this case, I’m referring specifically to cannabis oil, also called hemp oil and hash oil (though hemp oil could also refer to a pressed oil derived from hemp seeds which contains a relatively low amount of medicinally superior cannabinoids, namely THC. To avoid confusion I will refer to it only as cannabis oil).
Cannabis oil refers to a highly potent extract of cannabinoids from cannabis, especially THC, usually in the range of 40-90% purity (though there are claims of higher purity), in the form of a thick oil that can be taken daily. The same science discussed above applies to cannabis oil as the same cannabinoids are present, only with the oil they are in much higher concentrations. It is due to the increased potency in cannabinoids, specifically THC, that cannabis oil is the most medicinal and beneficial form of the medicine.
The use of cannabis oil became most prominent due to a documentary made by a man named Rick Simpson. The documentary is called ‘Run From The Cure,’ ( the word cure referring to the conventional cures for cancer, like chemotherapy. The documentary focuses on the science of the endocannabinoid system, how to make the oil and what to expect, doctor testimonials, research regarding cannabis’ effect on cancer, and testimonials from patients that have used cannabis oil to successfully cure their cancer.
Another story that is making ground breaking news is a story that is dubbed: Brave Mykayla. It is the story of Mykayla Comstock, a 7 year old girl from Oregon who successfully used medical marijuana, specifically cannabis oil, to fully cure her leukemia.
Additional information on Rick Simpson, Rick Simpson Oil (cannabis oil created using Rick Simpson’s simple method), and how to make cannabis oil yourself can be found on Rick Simpsons personal website: http://phoenixtears.ca/.
Cannabis oil is effective to an unprecedented degree, so says science and the people who have used it successfully to treat their cancer. Unfortunately, unless you are approved to use cannabis medically, it is incredibly expensive and potentially dangerous to procure due to its legal status. Something obviously needs to change, but what can be done? What’s the next step?
*Note: Although it does not specifically contain a discussion on cannabis oil, this exceptional video speaks extensively on the overall science of cannabis’ effects on the endocannabinoid system, presents testimonials from doctors and patients, and discusses various government funded/peer reviewed studies verifying cannabis’ extraordinary effects. It is the video I recommend to anyone even remotely interested in the subject, and is a great introduction to the plethora of research on the issue. It contains the following credible credits:
http://www.knowledgeoftoday.org
Dr. Robert Melamede, Ph.D.
Associate Professor and Biology Chairman
Biology Department at the University of Colorado
CEO and President of Cannabis Science
“Cannabinoids kill cancer cells in many cases, people are not aware of this”
Dr. Manuel Guzman, Ph.D.
Department of Biochemistry and Molecular Biology
Professor at the Complutense University, Madrid, Spain
“Cannabinoids have the effect of inducing death in cancer cells”
Dr. Prakash Nagarkatti, Ph.D. Vice President for Cannabinoid Research
University of South Carolina Columbia Distinguished Professor
“Cannabinoids can be used effectively as anti-cancer agents”
Dr. Sean McAllister CPMC Scientist
California Pacific Medical Center Research Institute http://thesethgroup.org/videos.html
“Cannabidiol inhibits aggressive breast cancers”
Dr. Donald Tashkin, M.D.
University of California, Los Angeles
Emeritus Professor of Medicine
Medical Director of the Pulmonary Function Laboratory
“THC actually has an anti-tumor effect”
Dr. Robert Sterner, M.D.
UCSD General Surgeon
Graduate of Harvard & UCLA
“Marijuana seeks out cancerous cells and preferentially kills them”
Dr. Jeffrey Hergenrather, M.D.
Addiction Medicine Specialist
President of the Society of Cannabis Clinicians
“There are multiple mechanisms of action in which cannabis kills cancer cells”
Dr. Bonni Goldstein, M.D.
Canna Centers, Medical Director
Cannabis Researcher and Scientist
“Cannabidiol has been found to make cancer cells commit suicide”
Dr. Josh Wurzer, Researcher
Laboratory Director, SC Laboratories
Cannabis Researcher and Scientist
“Health benefits attributed to THC is actually because of the CBD content”
What’s the Next Step?
It should now be clear by reading this report that cannabis and hemp remain illegal for utterly irrational reasons that are actually damaging society as a whole. Most importantly, cannabis should not be labeled a schedule 1 substance as it contains, at the very last, a substantial amount of medicinal value. This medicinal effect comes with the added bonus of having little to no danger of addiction, overdose, or biological harm; something that cannot be said about most other substances approved by the FDA. Even aspirin, a substance millions of people around the world pop like candy, kills 1000’s of people every year. Let’s not forget that the most popular pain killer in the world has been found to substantially increase heart attack risk.
A slew of studies…show diclofenac — sold under the brand names Voltaren, Cambia, Cataflam and Zipsor — is just as likely to cause a heart attack as the discredited painkiller Vioxx (rofecoxib), which was pulled from the U.S. market in 2004.
We have so many issues with modern medicine, yet a cheap (free if you grow it) natural, highly effective medicine/pain killer already exists in the form of cannabis. Why is it still only available to less than half the country, and only after jumping through extraordinary loopholes? Even more ludicrous, although medical cannabis users are practicing their legal state right, and moreover, the natural right to peacefully preserve their own lives, they are still labeled by the federal government as criminals deserving up to life sentences behind bars. This is alarmingly unreasonable and irresponsible decision making at best. At worst it is pure foolishness and downright criminal in itself.
Regardless of medicinal comparisons between substances, what is important is that people have as many medicinally effective substances available to them as possible, without interference from Big Brother. As Lynn Zimmer, PhD, former Professor Emeritus at the Queens College, City University, New York explains:
The question is not whether marijuana is better than existing medication. For many medical conditions, there are numerous medications available, some of which work better in some patients and some which work better in others. Having the maximum number of effective medications available allows physicians to deliver the best possible medical care to individual patients.
We recognize the legal hurdles and the hardships faced by patients fighting for the simple right to take a safe, proven to work medicine, but what is the next step? What must occur to end the madness?
The next step is to step out of the historical shadow of basing medical and political decisions on myths and rumors. More unbiased research needs to be performed on the effects of cannabis on each and every part of the human body and psyche. The DEA, FDA, and NIDA have made further legitimate research an ongoing uphill battle.
A pro-marijuana group lost its legal battle this week when a federal appellate court ruled that marijuana would remain a Schedule I drug, defined as having no accepted medical value and a high potential for abuse. The court deferred to the judgment of federal authorities, quoting the DEA’s statement that “the effectiveness of a drug must be established in well-controlled, well-designed, well-conducted and well-documented scientific studies…. To date, such studies have not been performed.
But guess who bears responsibility for the studies the court claims are not being performed? The DEA itself, which through its ultra-tight restrictions on cannabis made it nearly impossible for researchers to obtain the substance for study, as well as the National Institute for Drug Abuse, which controls the availability of the tiny quantity of research-grade cannabis that is federally approved for production.
In response to the DEA’s actions against sensible substance users, the LA Times accurately labeled the DEA as
a terrified and obstinate toddler when it comes to basic science.
Probably the most ridiculous aspect of the FDA’s behavior is that they approve of multiple synthetic cannabinoids which precisely mimic natural cannabinoids found in cannabis, especially THC. The only difference is that they and the pharmaceutical companies can add a few substances to the cannabinoid, call it a cocktail, and turn a significant profit on people in desperate need for something that works. So, synthetic cannabinoids which can be patented and sold at exorbitant rates are legal but naturally grown, free medicine containing the same exact cannabinoidal actions, as well as a wider range of medicinal benefits remains illegal. It doesn’t get much more hypocritical or shameless than that.
We have the ability to breed specified strains of cannabis, and create particular synthetic cannabinoids to meet the precise needs of patients. This incredible opportunity to create safe, effective, highly personalized medicine is stifled at the federal level, despite opposition from a majority of the US public.
The fact remains that Americans love cannabis. A recent survey of over 85,000 people revealed that at least 42% of Americans have tried cannabis. This is extremely surprising as only 20% of people in the Netherlands have tried cannabis, a country with extremely lax cannabis laws.
A second poll found that nearly 50% of Americans support legalizing cannabis, while 83% favor legalizing medical cannabis. Cannabis is such an American pastime that companies are planning to install cannabis vending machines in Washington and Colorado. Does this mean that 42% of Americans should be in prison, and 83% of Americans should be on the wanted list for supporting an act listed as a felony?
(*Percentages reflect any cannabis use during a person’s life for the stated ages in the stated year.)
http://www.dope-smoker.co.uk
Canada: 44.5% (ages 15+ in 2005)
United States: 42.4% (ages 14+ in 2002-2003)
New Zealand: 41.9% (ages 16+ in 2004-2005)
Denmark: 36.5% (ages 16-64 in 2005)
Australia: 33.5% (ages 14+ in 2007)
France: 30.6% (ages 15-64 in 2005)
United Kingdom: 29.6% (ages 14+ in 2004)
Italy: 29.3% (ages 15-64 in 2005)
Spain: 28.6% (ages 15-64 in 2005-2006)
Chile: 26% (ages 12-64 in 2009)
Germany: 24.5% (ages 18-59 in 2003)
Netherlands: 22.6% (ages 15-64 in 2005)
Czech Republic: 20.6% (ages 18-64 in 2004)
Scotland: 20.5% (ages 16-64 in 2004)
Austria: 20.1% (ages 15-64 in 2004)
Millions of people worldwide use cannabis for an endless list of reasons. Besides using it as a medicine, people all over the world responsibly use cannabis to experience:
Why are the DEA/FDA stalling? They raid innocent people’s homes, destroying families and jailing individuals for hyperbolic amounts of time. They go to all this effort to rid society of non-violent, victimless crimes. All this fear and war over a substance that they admit is beneficial (ie. allowing synthetic cannabinoids to be used medicinally and still sending medically grown cannabis to individuals). This is explicitly hypocritical and undoubtedly insane.
If the DEA/FDA are truly concerned over Americans’ safety, why are they not going after the truly dangerous substances. Research routinely finds that cannabis is strikingly safer than alcohol and tobacco within every measurable facet.
According to a 2006 United Kingdom government report, using cannabis is much less dangerous than tobacco, prescription drugs, and alcohol in social harms, physical harm, and addiction.
The scheduling system is nonsensical and has no clear logical basis for the large majority of listed substances.
Another important point is that through the legalization of cannabis, the economy could be booming! Here is a list of some examples of how cannabis legalization has already positively affected the economy, and how further legalization will improve the economy in the future:
Tobacco companies have the land to grow it, the machines to roll it and package it, the distribution to market it. In fact, some firms have registered trademarks, which are taken directly from marijuana street jargon. These trade names are used currently on little-known legal products, but could be switched if and when marijuana is legalized. during the run up to the 2010 election in which marijuana legalization was on the ballot in California, Altria took control of the web domain names AltriaMarijuana.com and AltriaCannabis.com. For those not in the know, Altria is the parent company of Phillip Morris, the manufacturer of Marlboro, Players, Benson & Hedges and many other popular brands of tobacco cigarettes.
We calculate that a reduction by one-half in the incarceration rate of non-violent offenders would lower correctional expenditures by $16.9 billion per year and return the U.S. to about the same incarceration rate we had in 1993 (which was already high by historical standards). The large majority of these savings would accrue to financially squeezed state and local governments, amounting to about one-fourth of their annual corrections budgets. As a group, state governments could save $7.6 billion, while local governments could save $7.2 billion.
Cannabis has the potential to change everything for the better. It could also help alleviate the health care crisis as Americans would be able to grow their own highly effective medicine. Let’s not forgot about the multitude of uses for hemp. It’s no wonder so many industries are lobbying against cannabis and hemp legalization including:
Vote! Voting is one of the best ways to enact change. It’s how Washington and Colorado were able to finally legalize cannabis.
Talk to your representatives. Send an email to your house representative and your state senators. Let them know how you feel, and how you think they should vote.
Do your own research. Alter your perceptions so that they are founded on evidence and scientific data.
Spread the world. Share this report or other relevant information you find and help educate others. Don’t be afraid to talk to people and tell them about what you’ve learned.
Don’t give up: people’s freedom and lives are at stake!
Final Thoughts
I would like to take the time to point out that this report’s aim is to argue why cannabis should be recognized as a medicine, and to thoroughly point out how incredible it is that it is not. Although I am admittedly in favor of it, I am not arguing for recreational use. Medicinal availability and options that work are the priorities here.
Virtually everything we encounter in life can be abused and unhealthily depended upon for happiness, be it video games, work, sex, masturbation, food, television, coffee, nail biting, reading, or even heavy metal. If you are going to use cannabis recreationally, use it responsibly, and don’t abuse it to the point of dependence. A relatively small amount of very heavy cannabis users do report withdrawal symptoms when attempting to stop smoking, but symptoms are extremely mild and usually involve difficulty sleeping, loss of appetite, and moodiness for 1-7 days. Regardless, this shows that despite the safety, a socially harmful dependence remains possible, as is the case with everything in life. Remember, cannabis should be used in moderation (or as directed by your physician if you are using it medicinally). Moderation is the key to happiness and health.
To put it simply, cannabis is not for everyone, but that does not mean people who safely and peacefully ingest cannabis should be seen as criminals.
A paradigm shift in information availability and critical thinking is occurring in humanity, an ubiquitous evolution on a global scale. We are growing out of outdated traditions. More and more often we are basing our decisions on fact and evidence, rather than on opinion and stipulation. My hope is that by reading this report you will be sufficiently equipped with the proper information to understand an aspect of the changes that are occurring all around you. Become part of the solution. Don’t just listen; wonder, research, evaluate, consider…and be always growing.
Even more amazingly, studies all around the world have concluded with exponentially growing empirical affirmation that cannabis completely and totally cures cancer. It additionally acts as a preventative, stopping cancer from ever coming back. Don’t believe me? Continue reading, or just ask the US government; they own the patent for cannabis as a successful cure and/or treatment for a whole array of medical conditions.
So why then is cannabis labeled as a schedule 1 drug, or in laymen terms, a dangerous, highly addictive substance devoid of any medical benefit? Tobacco has absolutely no medical benefits, is proven to cause cancer, is proven to kill hundreds of thousands of people worldwide, and is one of the most physically and psychologically addictive substances on the planet. However, tobacco, like alcohol, isn’t even scheduled. Additionally, cannabis is scheduled as even more dangerous, more addictive, and less medicinally beneficial then cocaine or methamphetamine, which are labeled as schedule 2 substances. As another example of the illogical scheduling process, psilocybin mushrooms, LSD, and DMT, which have been proven to be highly effective to cure cluster headaches as well as an invaluable tool in psychotherapy, are labeled as schedule 1 drugs despite these psychedelics having little to no addiction potential. Are you starting to see how silly this is? So what gives?
Let’s walk through this one step at a time. We are going to go over the historical use and legality of cannabis, the current legal status of cannabis around the world, the effects of keeping cannabis and other drugs illegal, and finally, the miraculous medicinal properties of cannabis. Feel free to jump around, but to gain a fully comprehensive understanding of this complex issue, I highly recommend reading all of this information.
Cannabis is a natural human pastime, embedded into our epigenetic expression. It was used for centuries as a form of relaxation, as a tool for meditation during religious ceremonies, and as a way to foster creativity. Additionally, hemp is one of the oldest domesticated plants known. Hemp was used in various industries, optimizing productivity, efficiency, and waste management Then one day, cannabis and hemp were suddenly seen as cesspools of sin originating from the pits of hell.
Both hemp and cannabis were made illegal for multiple reasons, but the most prominent reasons were due to money, ignorance, and irrational racism. All around the world cannabis and hemp were being criminalized simply by default; by tossing them in a category with substances that were highly addictive (opium, hashish, morphine, etc.). There was no consideration for each substance’s individual pros and cons, and certainly no empirical scientific basis. Anything with even the slightest amount of potential for addiction was just labeled together as a harmful/addictive substance, and that was that. The US took a similar approach.
In an attempt to make substance regulation laws more uniform, all states were encouraged to regulate cannabis in the same way, essentially handing over control to the federal level. Up until this point cannabis was still legal and available as a medicine; it was simply regulated while its recreational use was criminalized. Then along came Harry Anslinger, the future head of the Federal Bureau of Narcotics, and a nuclear bomb of lies, deceit and propaganda was dropped onto the US and the world at large.
There are 100,000 total marijuana smokers in the US, and most are Negroes, Hispanics, Filipinos, and entertainers. Their Satanic music, jazz, and swing, result from marijuana use. This marijuana causes white women to seek sexual relations with Negroes, entertainers, and any others.
…the primary reason to outlaw marijuana is its effect on the degenerate races.
Marijuana is an addictive drug which produces in its users insanity, criminality, and death.
Reefer makes darkies think they’re as good as white men.
Marihuana leads to pacifism and communist brainwashing.
You smoke a joint and you’re likely to kill your brother.
Marijuana is the most violence-causing drug in the history of mankind.
We recognize these claims as utterly ridiculous nowadays, but congress back in the day wasn’t very bright. I guess some things never change.
Anslinger and his buddies were also directly responsible for the propaganda video entitled “Reefer Madness,” depicting young men and women becoming violent, sex crazed, and downright insane after smoking cannabis. “Reefer Madness” was seen as a legitimate informational source at the time of its release and for many decades afterward. It is now shown to students as a form of retrospective humor. Anslinger used baseless scare tactics in an attempt to bolster criminalization laws in the US regarding cannabis, and even more astounding, industrial hemp, which can in no way get a person high.
What should you take out of this brief history lesson? Congress made cannabis(a great medicine) and hemp (a product that would revolutionize countless industries) illegal because of a silly, sensationalized, utterly unscientific movie shown to school children. They disregarded the claims made by experts and medical professionals. They ignored the pleas for rational thought and sensibility. They had no reason to make cannabis illegal, and still don’t. I guess that’s why times are changing so quickly!
Contemporary Legality
In the latter half of the 20th century, rational substance reform finally began to take a turn with actual long term medical/economic/political/social implications of each individual substance in mind. It became clear that the historical basis for keeping cannabis illegal is entirely political and has nothing to do with science. Just think, even main stream media and most countries around the world still refer to cannabis with a name spawned from mindless propaganda; marijuana.
People all around the world have begun to see that the war on drugs has completely failed in every way imaginable, actually leading to more drug use and significantly more violence worldwide. This is due to the fact that the war on drugs only fights the symptoms of a disease deeply ingrained into our society, and I’m not talking about drug use; I’m referring to gangs/organized drug cartels. In response to the effectiveness of incarceration on drug crimes, the Public Safety Performance Project found that:
Once incarcerated, drug dealers tend to be quickly replaced by new dealers and, as during the crack epidemic, the new recruits can be younger and more prone to violence than their predecessors. Thus while drug dealers no doubt deserve punishment, most leading researchers, and many law enforcement officials, now agree that incarcerating the foot soldiers in drug gangs, not to mention drug users, has a negligible impact on crime. Moreover, by creating job openings in drug-dealing organizations, it draws more people into criminal lifestyles and may in certain cases exacerbate crime.
More than 9.8 million people are held in penal institutions throughout the world, mostly as pre-trial detainees (remand prisoners) or as sentenced prisoners. Almost half of these are in the United States (2.29m), Russia (0.89m) or China (1.57m sentenced prisoners).
Taxpayers spent about $68.7 billion in 2008 to feed, clothe, and provide medical care to prisoners in county jails, state and federal prisons and facilities housing legal and illegal aliens facing possible deportation. From 1982 to 2002, state and federal spending on corrections, not adjusted for inflation, rose by 423%, from $40 to $209 per U.S. resident. Corrections spending, as a share of state budgets, rose faster than health care, education, and natural resources spending from 1986 to 2001. The average cost of housing a prisoner for a year was about $24,000 in 2005, though rates vary from state to state.
That incredible spending increase from 1982 to 2002 coincides precisely with the increase of drug arrests due to the failed ‘war on drugs.’ This is an especially important point to consider since drug offenses are almost entirely non-violent, and rehabilitation costs significantly less for tax payers.
Treatment delivered in the community is one of the most cost-effective ways to prevent such crimes and costs approximately $20,000 less than incarceration per person per year. A study by the Washington State Institute for Public Policy found that every dollar spent on drug treatment in the community yields over $18in cost savings related to crime. In comparison, prisons only yield $.37 in public safety benefit per dollar spent. Releasing people to supervision and making treatment accessible is an effective way of reducing problematic drug use, reducing crime associated with drug use and reducing the number of people in prison.
… the benefit to counties where private prisons are built and operated can be quite scant — some receive less than $2 per prisoner per day from the private prison operator…the federal government agreed to pay CCA [one of the largest private prison firms] almost $90 per day for each detained immigrant at a San Diego facility.
Today, private companies imprison roughly 130,000 prisoners and, according to one group, 16,000 civil immigration detainees in the United States at any given time. As states send more and more people to prison, they funnel ever greater amounts of taxpayer money to private prison operators. By 2010, annual revenues of the two top private prison companies alone stood at nearly $3 billion.
Many political leaders, heads of agencies, and medical professionals are also pointing out how ridiculous it is that extremely addictive, highly toxic substances like tobacco and alcohol go unchecked while a harmless substance like cannabis remains globally demonized. Ask yourself, if alcohol were discovered today would it even be legal? In the UK, the chief drug adviser Prof. David Nutt was fired for pointing out the dangers of alcohol and nicotine and further explaining that they are for more dangerous and harmful than cannabis. Another UK drug adviser recently resigned from his job in protest of David Nutt’s silencing.
It does not make sense from a prioritization point of view for us to focus on recreational drug users in a state that has already said that under state law that’s legal.
President Obama’s response was typical of all political speech; evasive and vague. While tokers all around the country take bets on the fed’s actions, there is a significant amount of pressure on the white house to legalize cannabis at the federal level. Various bills are being presented in Congress to repeal cannabis laws and broaden economic opportunities. Although there are steps you can take, like signing this petition to give states the right to regulate cannabis however they want, decisions and movement at the federal level remain slow and stagnant as usual.
So, countries all around the world along with a growing number of US states are decriminalizing cannabis for personal use, legalizing cannabis as a medicine (or entirely legalizing it), and the US government owns a patent on medicinal cannabis as well as supplies certain patients with medical cannabis for life. What’s all the hype over cannabis? It just so happens that cannabis is a wonder-drug; a miracle for millions; potentially billions.
The Endocannabinoid System
Cannabis is one of the most highly effective medicinal substances in the world. It has the power to treat and/or cure a countless number of illnesses and syndromes, including a whole array of different types of cancer. But how can a single substance have such an extraordinary effect on our biology? It all begins with the endocannabinoid system.
Because the discovery of the endocannabinoid system is relatively new, and despite there being over 12,000 scientific articles concerning the endocannabinoid system, there are still gaps in our understanding. There is still a significant amount of research that needs to be done, and educating people on the actual science of cannabis’ activity in the body will help to clear the smoke of ignorance and closed mindedness. Once people embrace the current research that is taking place, further research into more specific and particular roles of the endocannabanoid system will take off at lightning speed. What we do know is the following:
Endocannabinoids are the substances our bodies naturally make to stimulate these receptors. The two most well understood of these molecules are called anandamide and 2-arachidonoylglycerol (2-AG). They are synthesized on-demand from cell membrane arachidonic acid derivatives, have a local effect and short half-life before being degraded by the enzymes fatty acid amide hydrolase (FAAH) and monoacylglycerol lipase (MAGL).
Phytocannabinoids are plant substances that stimulate cannabinoid receptors. Delta-9-tetrahydrocannabinol, or THC, is the most psychoactive and certainly the most famous of these substances, but other cannabinoids such as cannabidiol (CBD) and cannabinol (CBN) are gaining the interest of researchers due to a variety of healing properties. Most phytocannabinoids have been isolated from cannabis sativa, but other medical herbs, such as echinacea purpura, have been found to contain non-psychoactive cannabinoids as well.
The information above focuses on the two most well known endocannabinoids in the body, as well as the most well known cannabinoids in cannabis, but there are far more. Cannabinoids are split into three categories:
It is through the encocannabinoid system that cannabis is able to perform its magic. Cannabis has the ability to treat and/or cure a constantly growing list of illnesses, including cancer. Dependent on the individual and the type of cannabinoid used, most types of cancer have been observed responding positively to the introduction of cannabis in the system, including cancer found in the breast, prostate, lung, thyroid, colon, skin, pituitary gland, ovary, pancreas, as well asmelanoma, leukemiaandmore! The cannabinoids in cannabis act through the body’s natural endocannabinoid system to cure and/or treat cancer in several ways, the most prominent and well researched being:
One of the greatest benefits of cannabis as medicine is that it stimulates and acts in harmony with a system that is already present throughout the body. Instead of prescribing five or more different, highly addictive pills to treat various symptoms, and additional pills to treat the endless side effects (often worse than the illness itself) of all the pills, doctors are able to use cannabis and the cannabanoids within it, as a single, natural medicinal source without any physical addiction potential and little to no harmful side effects. Plus, don’t forget, it is impossible to overdose on.
Cannabis Cures Everything Else
Along with treating various forms of cancer, cannabis can be used to treat a constantly growing list of other diseases and syndromes as well. It may even slow the aging process. Additionally, the cannabinoids found in cannabis are exceptional anti-oxidants and neuroprotectants. It is such a remarkable substance that it is able to treat seemingly opposite illnesses simultaneously, like obesity and eating disorders/malnutrition. Again, the key is the activation and involvement with the endocannabinoid system. Cannabis has shown results ranging from promising potential to revolutionary effectiveness in curing and/or treating:
(*Note: each of these words link to an individual study)
It is because the cannabinoids in cannabis are so influential on the endocannabinoid system, a system that spans every part of our body, that they are able to have such an effective, overarching, revolutionarily positive effect. Keep in mind that the above is what researchers have found with limited funds, little time, and immense legal obstacles. The golden age of cannabis research hasn’t even started yet.
What the Critics Have to Say
(And Why They’re Wrong…)
On the flip side, critics are quick to point out the consistently noted dangers of cannabis ingestion. These are the same arguments that have been used for decades. They remain aggressively debated without compromise, despite decades of rational evidence suggesting falsity and fallacy. The seemingly valid concerns regarding cannabis use that top the critics’ list are: the gateway drug theory, short-term memory loss, psychosis, decreased intelligence, harm from cannabis smoke, depression, an elevated heart rate, and worries over driving while high. Let’s allow science and logic to save the day, shall we?
Gateway Drug
Many critics of cannabis use claim that cannabis is a gateway to harder and more persistent drug use. They are implying that if a person uses cannabis, recreationally or medically, they are more likely to use dangerous drugs like cocaine (again, ironically listed as a schedule 2 drug) or heroin. Although multiple studies have found that cannabis users are more likely than non-users to engage in the use of more ‘hardcore’ substances (meaning higher addiction potential and/or more biologically detrimental), there are endless holes in this argument.
Much of their [US drug-policy leaders] rhetoric about marijuana being a ‘gateway drug’ is simply wrong. After decades of looking, scientists still have no evidence that marijuana causes people to use harder drugs. If there is any true ‘gateway drug,’ it’s tobacco.
Alcohol and tobacco are more accessible and far more likely to be used by teens, consequently making those substances more likely to lead to further drug use. As stated by Elders, they are the true gateway drugs. In one of the most highly credible and sourced assessments on the science of drug use, the Institute of Medicine stated that:
In fact, most drug users do not begin their drug use with marijuana–they begin with alcohol and nicotine, usually when they are too young to do so legally…
There is no evidence that marijuana serves as a stepping stone on the basis of its particular physiological effect.
Starting to see the trend here? Alcohol and tobacco are far more dangerous and addictive than cannabis. If the gateway drug theory did have any legitimacy, it would have to be applied to alcohol and nicotine, two completely legal substances, before it could be attributed to any other substance.
The best analogy I’ve ever encountered for the ridiculousness of the gateway drug theory comes from Lynn Zimmer, PhD, Professor Emeritus at Queens College at the City University of New York:
In the end, the gateway theory is not a theory at all. It is a description of the typical sequence in which multiple-drug users initiate the use of high-prevalence and low-prevalence drugs.
A similar statistical relationship exists between other kinds of common and uncommon related activities. For example, most people who ride a motorcycle (a fairly rare activity) have ridden a bicycle (a fairly common activity). Indeed, the prevalence of motorcycle riding among people who have never ridden a bicycle is probably extremely low. However, bicycle riding does not cause motorcycle riding, and increases in the former will not lead automatically to increases in the latter.
Nor will increases in marijuana use lead automatically to increases in the use of cocaine or heroin.
If we overly criminalize behaviors like marijuana use among teens, this could interfere with opportunities for education and employment later on, which, in turn, could be creating more drug use.
The gateway drug theory is weak and unfounded. It is in fact not a credible theory at all. It has no place in the realm of science.
Decreased Intelligence
It is a propaganda technique that we have been hearing for nearly the entire 20th century and it continues into the 21st century; cannabis makes you stupid, a loser, a burnout.
While there is clear evidence that cannabis, like other substances, alters perception and brain function, there is no evidence that cannabis alters brain function in a purely negative way. Additionally, there is absolutely zero evidence that the biological effects of cannabis are permanent. On the contrary, science tells us that all of the consistently noted negative biological aspects of cannabis are entirely temporary.
According to Igor Grant, MD, Executive Vice Chairman at the University of California, San Diego Department of Psychiatry:
Smoking marijuana will certainly affect perception, but it does not cause permanent brain damage. ‘The findings were kind of a surprise. One might have expected to see more impairment of higher mental function. Other illegal drugs, or even alcohol, can cause brain damage…
If we barely find this tiny effect in long-term heavy users of cannabis, then we are unlikely to see deleterious side effects in indivduals who receive cannabis for a short time in a medical setting…
If it turned out that new studies find that cannabis is helpful in treating some medical conditions, this enables us to see a marginal level of safety.
Government experts now admit that pot doesn’t kill brain cells.
This myth came from a handful of animal experiments in which structural changes (not actual cell death, as is often alleged) were observed in brain cells of animals exposed to high doses of pot. Many critics still cite the notorious monkey studies of Dr. Robert G. Heath, which purported to find brain damage in three monkeys that had been heavily dosed with cannabis. This work was never replicated and has since been discredited by a pair of better controlled, much larger monkey studies, one by Dr. William Slikker of the National Center for Toxicological Research [William Slikker et al., ‘Chronic Marijuana Smoke Exposure in the Rhesus Monkey,’ Fundamental and Applied Toxicology 17: 321-32 (1991)] and the other by Charles Rebert and Gordon Pryor of SRI International [Charles Rebert & Gordon Pryor – ‘Chronic Inhalation of Marijuana Smoke and Brain Electrophysiology of Rhesus Monkeys,’International Journal of Psychophysiology V 14, p.144, 1993].
Neither found any evidence of physical alteration in the brains of monkeys exposed to daily doses of pot for up to a year.
The surprising truth is that cannabis actually promotes the creation of new neurons in hippocampal regions of the brain, the part of the brain most responsible for memory. Xia Zhang, an expert at the Neuropsychiatry Research Unit, Department of Psychiatry, at the University of Saskatchewan in Canada along with other medical researchers, points out that cannabis is the only illicit drug ever found to promote the creation of brain cells:
We show that 1 month after chronic HU210 [high-potency cannabinoid] treatment, rats display increased newborn neurons [brain cell growth] in the hippocampal dentate gyrus [a portion of the brain] and significantly reduced measures of anxiety- and depression-like behavior.Thus, cannabinoids appear to be the only illicit drug whose capacity to produce increased hippocampal newborn neurons is positively correlated with its anxiolytic- [anxiety reducing] and antidepressant-like effects.
College students who smoke cannabis demonstrate comparable or even higher grades than their cannabis abstinent classmates, and are more likely to pursue a graduate degree.
The short answer is yes, cannabis alters your mind and body, like any other substance in the world, but it does not make you stupid (certainly you’re not going to claim any of these highly successful cannabis-users are stupid), and all of the physiological and psychological effects are temporary.
Critics of cannabis use argue that memory loss, especially short-term memory loss, occurs more prominently in cannabis smokers. They also claim that it is a permanent effect. All of these claims are either exaggerated or wrong. We’ve already discussed how all the effects of cannabis ingestion are completely temporary; the same applies to memory.
To begin, it is true that cannabis has a noticeable effect on short-term memory as well as working memory, while the user is under the influence. Cannabis affects working memory through the mechanisms stated above, by encouraging neurogensis, or the creation of neurons, in the hippocampus region of the brain. Although this has a positive effect on memory overall, it disrupts short-term memory while the user is ‘high’ by creating ‘noise’ in the hippocampus. These effects are detectable at least 7 days after heavy cannabis use,
but appear reversible and related to recent cannabis exposure rather than irreversible and related to cumulative lifetime use.
Furthermore, after extensively studying cannabis use, lead researcher and Harvard professor Harrison Pope came to the conclusion that:
From neuropsychological tests chronic cannabis users showed difficulties, with verbal memory in particular, for ‘at least a week or two’ after they stopped smoking.Within 28 days, memory problems vanished and the subjects ‘were no longer distinguishable from the comparison group.’
These tests affirm that the physio/psychological effects of cannabis are temporary and reversible.
As for the seriousness of the temporary effects on short-term memory, studies have found that the effect is negligible. Researchers from the University of California, San Diego School of Medicine headed by Dr. Igor Grant analyzed data from 15 previously published controlled studies involving 704 long-term cannabis users and 484 nonusers and found that:
long-term cannabis use [is] only marginally harmful on the memory and learning. Other functions such as reaction time, attention, language, reasoning ability, perceptual and motor skills [are] unaffected. The observed effects on memory and learning, [show] long-term cannabis use [causes] ‘selective memory defects’, but that the impact [is] ‘of a very small magnitude.’
In fact, rather than having deleterious effects on memory, Ohio State University scientists have shown that
Research supports this claim as past studies have revealed that cannabinoid receptors stimulated by cannabinoids in cannabis act as an anti-inflammatory agent and serve to improve memory in old rats.
Surprisingly, recent research into the activity of the hippocampus suggests that the key to a good memory is forgetting. Think of the brain as a computer with enormous hard drive space. Despite this incredible amount of storage, it is still finite. The more memories our brains create, the harder it is for our working memory to properly remember and recall. In this way, forgetting a few things actually isn’t a bad thing. It is in fact highly beneficial overall.
Another important point is that different cannabinoids found in cannabis affect memory centers in the brain in remarkably different ways. Through further legalization, scientists will have the freedom to perform more extensive research, while growers will have the opportunity to create strains of cannabis that have an even more minimal effect on the memory centers of the brain.
These studies reveal that in the short run, short-term and working memory are disrupted by the ingestion of cannabis by creating new neurons in the memory centers of the brain. These additional neurons disrupt working memory by acting as additional ‘noise’ to the active, recalling mind. These short-term memory lapses are completely temporary though, and in the long run the brain is actually left with additional neurons and a more expansive memory center. To use the analogy of a computer again, think of heavy-cannabis ingestion as a temporary lapse in primary memory functionality for the sake of upgrading the storage capabilities of secondary memory.
Elevated Heart Rate
It is true that many cannabis users describe symptoms of panic and consequently an elevated heart rate, especially during their first time trying cannabis. What still remains debated is whether cannabis itself biologically causes heart rate to increase.
The most well known study done on the correlation between cannabis and heart rate, and subsequently the only truly credible and widely used study, is one performed by a man named Dr. Murray A. Mittleman. Mittleman’s study focused on:
information on cannabis use from 3,882 middle-aged and elderly patients who had suffered heart attacks. A total of 124 patients were identified as current users, including 37 who reported smoking the drug up to 24 hours before their attack, and nine who had used it within an hour of experiencing symptoms.
Mittleman’s conclusion was that the first hour after taking cannabis heart attack risk is 4.8 times higher than during periods of non-use. In the second hour, the risk drops to 1.7 times higher. According to Mittleman this was the first study to document that smoking cannabis could trigger a heart attack, but that the trigger mechanism remained unknown. So what’s the issue with this constantly cited study?
Besides the fact that any type of smoke entering the lungs produces the same effect (it is not necessary and not medicinally optimal to smoke cannabis, a subject that is covered later in this report), Dr. Lester Grinspoon, who is one of the world’s foremost cannabis researchers as well as Associate Professor Emeritus of Psychiatry at Harvard Medical School and a former senior psychiatrist at the Massachusetts Mental Health Center in Boston for 40 years, explains why this study should be dismissed. Dr. Grinspoon tells an interviewer, in response to Mittleman’s study:
..let me say that since 1967 there have been numerous reports and studies, each of which the American media has blown out of all proportion, stating one or another supposed ill effect of marijuana use. I can list them, if you’d like. ‘Increase in the size of the ventricles, decrease in testosterone, destruction of chromosomes.’ All were front-page stories, none of them have ever been replicated. In other words, they didn’t pan out scientifically. Of course, the studies that contradicted them ended up on page 31 or thereabouts, if they got mentioned at all… I would point out that out of 3,882 patients, we’re talking about 9 who used marijuana within an hour of the onset of a heart attack. That’s around 0.2%. By sheer mathematics, given that people sleep eight hours per day or so, we can deduce that 6.7% of those patients emptied their bowels within an hour of onset. It’s incredible to me that the numbers here could be said to constitute a significant risk factor.
So, as is typical of the main stream media, a report was utterly sensationalized and relatively negligible data was heralded as proven truth. Dr. Grinspoon elaborates on the shortcomings of the study by reminding the interviewer that:
[Mittleman] put that increase [in heart rate] at 40 beats per minute. In truth, that number is closer to 20 beats per minute, which is probably consistent with running up the stairs in one’s house...I blame the media far more than I do Dr. Middleman. I read his abstract, and in its conclusion he cautioned against making too much of the data…in 1997, Kaiser Permanente did a large-scale study which included more than 65,000 admitted marijuana users, and they could not demonstrate any impact of marijuana use on mortality. If marijuana use really was a significant risk factor for heart attack, it is hard to believe that it didn’t turn up there. Again, I’m not saying that there is absolutely no risk demonstrated here. But given the history of the research since 1967, I’d be surprised if these findings don’t go down the same chute as all of the other front-page scare stories.
It’s really not that hard to believe. We have seen the same baseless scare tactics take place 20 years ago, 40 years ago, 60 years ago, 100 years, and more!
With regards to actual significant scientific data, cannabis has in fact been shown (as stated in the ‘Cannabis Cures Everything’ section of this report) to treat and protect the heart, as well as help prevent heart disease through the interaction with the endocannabinoid system of the heart and surrounding regions of the body. It is consequently a likely tool for fighting and preventing obesity (along with hemp seeds). The science is still emerging, but what little research exists strongly suggests that cannabis will serve an extremely positive role in keeping the heart healthy in the future.
The single study that is consistently used to argue that cannabis poses a danger to cardiovascular health is far from significant and only became prominent through sensationalized media. Repeat studies suggest the cannabinoids found in cannabis play a pivotal role in cardiovascular health and the prevention of heart disease.
Psychosis
An historically major issue concerning cannabis is the worry that it may induce schizophrenic symptoms or intensify various forms of latent schizophrenia. The subjective experience of ingesting cannabis is highly personal and varies greatly among users around the world. Common experiences include:
Greater enjoyment of food taste and aroma
blogs.sfweekly.com
An enhanced enjoyment of music
A greater enjoyment of comedy and humor
Distortions in perception of time and space
Short-term memory loss
Improved long-term memory recall
Creative thinking
New perspectives
Increased libido
Elevated mood
Heightened sensitivity to external stimuli
Relaxation
At extremely high doses common experiences include:
Altered body image
Auditory/visual illusions
Hallucinations (extremely rare)
Mild dissociation of mind and body
Panic attacks
Paranoia
While the vast majority of the effects of cannabis are viewed as positive, panic attacks and paranoia are obviously unwanted. Between 20 and 30 percent of recreational users experience intense anxiety and/or panic attacks after smoking cannabis.
While these symptoms usually occur due to thoughts of legal ramification for ingesting cannabis, exaggerated worry over a thought process, or general anxiousness over trying something new, it has been reported that the symptoms can happen spontaneously as well. It is possible and plausible that these symptoms could lead to greater and more persistent symptoms of psychosis. However, there are multiple aspects of the psychosis worry that needs to be discussed.
First, through our increasing knowledge of cannabinoids and the role they play on the endocannabinoid system, researchers have discovered that certain cannabinoids have a marginally stronger effect than others with regards to producing hallucinations delusions, and subjective psychological stress.
While the THC (the most psychoactive cannabinoid found in cannabis) offers incredible physio/psychological health benefits, it has been linked to being the sole culprit of producing more schizophrenia-like symptoms.
When comparing multiple subjects under the influence of only THC, a mixture of THC and CBD (cannabidiol), and no cannabinoids, researchers found that only THC produced subjectively negative psychological effects. The subjects with no additional cannabinoids in their system and the subjects with the mixture of THC and CBD both experienced a nearly identical psychological effect. The only major difference was that the subjects who had ingested the mixture reported less anhedonia (unable to experience pleasure) then the other two groups. The researchers concluded that if anything, their research highlighted
the importance of distinguishing between different strains of cannabis.
Once we break cannabis down into its component cannabinoids it is easy to see why users describe such incredibly varied experiences. Cannabidiol is extremely effective in treating and preventing symptoms of schizophrenia, as research continues to suggest. Many researchers believe that cannabis legalization will herald a revolution in the treatment of various psychological disorders, including schizophrenia. According to a 2005 double-blind study analyzing the antipsychotic effects of cannabidiol, researchers found that:
cannabidiol treatment was accompanied by a significant increase in serum anandamide levels, which was significantly associated with clinical improvement. The results suggest that inhibition of anandamide deactivation may contribute to the antipsychotic effects of cannabidiol potentially representing a completely new mechanism in the treatment of schizophrenia.
Other studies on the topic affirm that many subjects report
A group of Dutch scientists say that there is no proof that cannabis induces schizophrenia. These findings will be embarrassing for the Dutch government, which has been bearing down on Marijuana Coffee Shops saying the drug induces schizophrenia.
The truth is that much of the research done thus far has been skewed and largely unscientific. Under proper guidance, and using the correct strains, researchers all around the world agree that cannabis is a wonderfully effective psychotropic medication. Researchers discussed the consistently shown promise and proof of cannabis as an effective psychotropic medication in the British Journal of Psychiatry:
I considered Arseneault et al‘s (2004) search for evidence of the association between cannabis and psychosis as quite skewed. They did not explore the evidence regarding positive, therapeutic or beneficial psychoactive effects of cannabis in mental health in the context of appropriate, rational and clinical usage…Signalling, mostly inhibitory, suggests a role for cannabinoids as therapeutic agents in central nervous system disease where inhibition of neurotransmitter release would be beneficial. Evidence suggests that cannabinoids inhibit the neurotransmitter glutamate, counteract oxidative damage to dopaminergic neurons and may be potent neuroprotective agents (Croxford, 2003)…knowing [cannabis’] potent neuroprotective function, its potential role in psychiatric practice should not be discarded lightly.
The most important thing to remember is that symptoms of schizophrenia generally (nearly always) precede cannabis use. Schizophrenia and general psychosis have far more to do with genetic make up than anything else (refer to the graph).
Research regarding the connection between cannabis and psychosis, especially symptoms of schizophrenia, remains historically lacking and skewed with regards to component cannabinoids in cannabis. Cannabis produces highly varied subjective experiences, and research has revealed that each cannabinoid within cannabis has a markedly different effect on individuals. Multiple recent studies have shown that cannabis, specifically the cannabinoid CBD, is a highly effective agent in treating schizophrenia and other psychological disorders. Most importantly, symptoms of schizophrenia precede cannabis use in the vast majority of cases. There is currently no clear evidence that cannabis is directly responsible for causing psychosis and schizophrenic symptoms in users.
Depression
This is one of the most commonly used arguments against the use of cannabis as a form of medicine or recreation. Like the psychosis argument debunked above, the depression argument is always portrayed in a skewed and exaggerated fashion. The most important thing to remember as we discuss this is that correlation does not imply causation.
forum.grasscity.com
It is well known that many already depressed individuals (ranging from mild to incapacitating depression) use cannabis as a form of self-medication. This often takes place after finding no success with taking a whole slew of expensive, addictive, and biologically destructive prescription drugs handed out by the oh so helpful DSM devotees.
Over 4400 adult internet users [who] completed The Center for Epidemiologic Studies Depression scale and measures of marijuana use. We employed an internet survey in an effort to recruit the most depressed and marijuana involved participants, including those who might prove unwilling to travel to the laboratory or discuss drug use on the phone or in person. We compared those who consumed marijuana daily, once a week or less, or never in their lives. Despite comparable ranges of scores on all depression subscales, those who used once per week or less had less depressed mood, more positive affect, and fewer somatic complaints than non-users. Daily users reported less depressed mood and more positive affect than non-users. The three groups did not differ on interpersonal symptoms.
Cannabis users, whether they ingested the substance less than once a week or every day, reported far less depressive symptoms and far more happiness and satisfaction than non-users. The study goes on to say that:
The media continues to report links between marijuana and depression. In a recent review, Degenhardt, Hall, and Lynskey (2003) identified a modest relationship only among problematic users. Many studies show no link between cannabis and depression despite appropriate statistical power, measurement, and design (Fergusson & Horwood, 1997; Fergusson, Lynskey, & Horwood, 1996; Green & Ritter, 2000; Kouri, Pope, Yurgelun-Todd, & Gruber, 1995; McGee, Williams, Poulton, & Moffitt, 2000; Musty & Kaback, 1995; Rowe, Fleming, Barry, Manwell, & Kropp, 1995). One neglected source of depression among marijuana users may stem from medical use. Separate analyses for medical vs. recreational users demonstrated that medical users reported more depressed mood and more somatic complaints than recreational users, suggesting that medical conditions clearly contribute to depression scores and should be considered in studies of marijuana and depression. The data suggests that adults apparently do not increase their risk for depression by using marijuana.
Just like we discussed in all of the other arguments, the public only sees what the media picks and chooses to show, which is usually negligible data that has been exaggerated and skewed to fit their hype. The previous study also brought up an excellent point that has never been discussed before: are the results of studies concerning cannabis and depression that get aired by main stream media corrupted by reports of depression that originate from medical suffering? The use of cannabis is so wide spread around the world, especially in the US, that it should not be discounted.
After adjusting for differences in baseline risk factors of marijuana use and depression, past-year marijuana use does not significantly predict later development of depression.
Finally, in a longitudinal study completed in 2009 regarding cannabis and suicide,researchers found that:
Although there was a strong association between cannabis use and suicide, this was explained by markers of psychological and behavioural problems. These results suggest that cannabis use is unlikely to have a strong effect on risk of completed suicide, either directly or as a consequence of mental health problems secondary to its use.
The depression argument is false in many of the same ways as the psychosis argument. In the vast majority of cases depressive behavior precedes cannabis use. Additionally, in most cases where cannabis is used to self-treat depression it is found to be successful. Cannabis is a clear biological antidepressant and exhibits incredible therapeutic properties. Depression is highly subjective and everyone experiences it differently. The truth is that in multiple studies both light and heavy cannabis users report far less depressive symptoms than non-users. There is no evidence whatsoever that cannabis use predicts or causes depression. Many depressed people use cannabis and report positive results far more often than people using contemporarily prescribed prescription medication.
lfp-blog.com
Driving While Stoned
(*Note: this report does not advocate driving while under the effects of any substance, including cannabis. The aim of this section is to view the credible findings on how cannabis affects drivers.)
cannabis impairs driving behavior. However, this impairment is mediated in that subjects under cannabis treatment appear to perceive that they are indeed impaired. Where they can compensate, they do.
Despite biological theories for how cannabis might potentially affect a driver, experiments using driving simulations in the lab find that:
drivers who drank alcohol overestimated their performance quality whereas those who smoked marijuana underestimated it. Perhaps as a consequence, the former invested no special effort for accomplishing the task whereas the latter did, and successfully. This evidence strongly suggests that alcohol encourages risky driving whereas THC encourages greater caution, at least in experiments.
The [findings] contrast with results from many laboratory tests, reviewed by Moskowitz (1985), which show that even low doses of THC impair skills deemed to be important for driving, such as perception, coordination, tracking and vigilance. The present studies also demonstrated that marijuana can have greater effects in laboratory than driving tests. The last study, for example showed a highly significant effect of THC on hand unsteadiness but not on driving in urban traffic.
It is apparent that despite multiple laboratory studies displaying favorable results, real world driving tests are even more positive. When we actually test the effects of cannabis on drivers in the real world, we see very little safety issues, if any at all.
Drivers under the influence of cannabis, unlike alcohol, realize they are under the effects of a substance and successfully compensate for their altered state of mind by driving slower and by giving themselves more space between other vehicles. One of the first actual road tests with cannabis studies drivers in the lab, on the highway, and in congested urban areas. The results affirmed that as far as cannabis’ effect on actual driving performance:
Driving quality as rated by the subjects contrasted with observer ratings. Alcohol impaired driving performance according to the driving instructor but subjects did not perceive it; marijuana did not impair driving performance but the subjects themselves perceived their driving performance as such….Thus there was evidence that subjects in the marijuana group were not only aware of their intoxicated condition but were also attempting to compensate for it…drivers become overconfident after drinking alcohol…and more cautious and self critical after consuming low THC doses by smoking marijuana.
Drivers under the effects of cannabis pay more attention to the road; drive more slowly, and leaving themselves more room between other cars.
The truth is that alcohol is a far more serious problem than cannabis when it comes to driving. Studies performed from 1982 to 1998 demonstrate time and time again that alcohol is significantly more dangerous than cannabis on the road. Alcohol use is also far more prevalent in crash statistics.
Blood and/or urine from fatally injured drivers in Washington State were collected and tested for the presence of drugs and alcohol. Drug and/or alcohol use was a factor in 52% of all fatalities. Among single vehicle accidents, alcohol use was a factor in 61% of cases versus 30% for multiple vehicle accidents. Drugs most commonly encountered were marijuana (11%), cocaine (3%), amphetamines (2%), together with a variety of depressant prescription medications.
The study even found that it was far less likely to find alcohol in a person’s system in the presence of cannabis, implying that cannabis use lessened the prevalence of alcohol use on the road:
Trends noted included an association of depressant use with higher blood alcohol levels, while marijuana use was associated with lower blood alcohol levels.
With regards to comparisons between cannabis and illicit substances overall, Accident Analysis & Prevention, a peer-reviewed journal, reported in its July 2004 article titled “Psychoactive Substance Use and the Risk of Motor Vehicle Accidents,” by K.L.L. Movig, et al.:
The objective of this study was to estimate the association between psychoactive drug use and motor vehicle accidents requiring hospitalization.
The risk for road trauma was increased for single use of benzodiazepines and alcohol…High relative risks were estimated for drivers using combinations of drugs and those using a combination of drugs and alcohol. Increased risks, although not statistically significant, were assessed for drivers using amphetamines… No increased risk for road trauma was found for drivers exposed to cannabis.
The largest study ever done linking road accidents with drugs and alcohol has found drivers with cannabis in their blood were no more at risk than those who were drug-free. In fact, the findings by a pharmacology team from the University of Adelaide and Transport SA showed drivers who had smoked marijuana were marginally less likely to have an accident than those who were drug-free. A study spokesman, Dr Jason White, said the difference was not great enough to be statistically significant but could be explained by anecdotal evidence that marijuana smokers were more cautious and drove more slowly because of altered time perception. The study of 2,500 accidents, which matched the blood alcohol levels of injured drivers with details from police reports, found drug-free drivers caused the accidents in 53.5 per cent of cases. Injured drivers with a blood-alcohol concentration of more than 0.05 per cent were culpable in nearly 90 per cent of accidents they were involved in. Drivers with cannabis in their blood were less likely to cause an accident, with a culpability rate of 50.6 per cent. The study has policy implications for those who argue drug detection should be a new focus for road safety. Dr White said the study showed the importance of concentrating efforts on alcohol rather than other drugs.
The BBC and CNN both filmed their own research on the actual effects of cannabis on driving ability. The BBC study focused on a single driver and found that he actually drove better while ‘high’; driving more cautiously and paying more attention to the driving test. The CNN study was a bit more extensive and controlled.
The study, conducted in Washington where recreational cannabis use is legal, focused on 3 volunteers who drove under the effects of different amounts of cannabis. They drove alongside a driving instructor with drug recognition experts (police officers with specific drug recognition training) watching them from outside the vehicle. The volunteers included a heavy daily user, a weekend user, and an occasional user. Even at 7x the legal limit of driving under the influence, 5x the legal limit, and 4x the legal limit respectively, all of the volunteers passed their driving tests, received positive reviews from the driving instructor, and would not have been pulled over by the drug recognition experts.
It’s just safer to drive under the influence of marijuana than it is drunk….Drunk drivers take more risk, they tend to go faster. They don’t realize how impaired they are. People who are under the influence of marijuana drive slower, they don’t take as many risks.
From a theoretical point of view it makes sense that people would be concerned over potential risks of ‘driving while stoned.’ However, the research speaks for itself. Laboratory and real world test results have confirmed time and time again that cannabis does not have a detrimental effect on driving ability. People under the effects of cannabis, unlike alcohol, realize their altered state of mind and compensate successfully for it. In most instances cannabis users drive more safely; driving slower, paying more attention to the road, and remaining more cautious and vigilant. Cannabis does not pose any serious danger to drivers or anyone else on the road.
atheistfoundation.org.au
Cannabis Smoke and Lung Damage
patients4medicalmarijuana.wordpress.com
There are endless reports that claim cannabis harms the lungs and bronchial airways, as well as increasing the risk of lung cancer. What you’ll quickly notice though is that the studies these reports are quoting from are completely theoretical studies based on comparisons with cigarette smoke, as opposed to actual findings from research. Additionally, they only focus on one mode of cannabis ingestion, one that destroys many of the medical benefits of cannabis; smoking.
It is true that there are over 50 potentially carcinogenic substances found in cannabis. Additionally, because smoked cannabis is not completely dry and is smoked without a filter, there is roughly 4 times more tar than the amount found in cigarettes. One can see why studies would speculate that cannabis may increase the risk of lung cancer. As usual, when you look at the actual science, the opposite is true.
First of all, there is currently not a single known case of cancer originating from the ingestion of cannabis. As stated numerous times in this report, there has never been a death that cannabis was directly responsible for.
A study in 2005, the largest ever conducted of its kind, left Donald Tashkin, a pulmonologist at UCLA‘s David Geffin School of Medicine, scratching his head. Tashkin and his research team had hypothesized an association between cannabis and lung cancer, but even after 30 years of observing thousands of subjects they were unable to find a connection between cannabis and lung cancer.
We hypothesized that there would be a positive association between marijuana use and lung cancer, and that the association would be more positive with heavier use. We expected that we would find that a history of heavy marijuana use – more than 500 to 1,000 uses – would increase the risk of cancer from several years to decades after exposure to marijuana. What we found instead was no association at all, and even a suggestion of some protective effect.
kushsmoke.com
The heaviest users in Tashkin’s study smoked more than 60 joint-years worth of marijuana, or more than 22,000 joints in their lifetime. Moderately heavy users smoked between 11,000 and 22,000 joints.
That’s an enormous amount of marijuana [however] in no category was there any increased risk, nor was there any suggestion that smoking more led to a higher odds ratio. There was no dose-response, not even a suggestion of a dose response, and in all types of cancer except one, oral cancer, the odds ratios were less than one. This is the largest case-control study ever done, and everyone had to fill out a very extensive questionnaire about marijuana use. Bias can creep into any research, but we controlled for as many confounding factors as we could, and so I believe these results have real meaning.
That being said, Dr. Tashkin wisely notes:
It’s never a good idea to take anything into your lungs, including marijuana smoke.
Smoke does not belong in your lungs, and just as this report does not advocate driving while under the effects of cannabis, it equally does not recommend smoking cannabis. What this report does suggest is using a vaporizer, cooking the cannabis into food, or making a cannabis oil. All of these methods make this entire argument irrelevant as they do not involve any form of smoke.
The media has bombarded the public with seeming ‘proof’ that cannabis leads to lung cancer. The truth is that all of this ‘proof’ has been entirely speculative. Despite cannabis smoke containing carcinogens and up to 4 times more tar than the amount found in cigarettes, long term studies confirm that there is no increased risk of lung cancer from smoking cannabis. On the contrary, the cannabinoids found in THC work to fight against cancer and even protect healthy cells. Most importantly, because cannabis can be ingested in many ways that don’t involve smoke, this entire argument is irrelevant.
Cannabis Oil: Run From the Cure
The most medicinally beneficial way to ingest cannabis is by making a high potency cannabis oil. It should be clear now from this report that cannabis is far more effective than conventional medicine for a near-endless variety of ailments. This is especially true for cancer.
The point is, no matter what type of conventional medicine you use, your chances of survival are bleak, and the side effects are horrendous. On the other hand, there is a medicine available that has been proven to completely cure cancer in the majority of cases, as well as having little to no adverse side effects. Additionally, it is as non-toxic as a substance can get, and is impossible to overdose on. Plus, it focuses on treating the side effects of cancer along with the cancer itself. At this point, you recognize that I’m referring to cannabis, but in this case, I’m referring specifically to cannabis oil, also called hemp oil and hash oil (though hemp oil could also refer to a pressed oil derived from hemp seeds which contains a relatively low amount of medicinally superior cannabinoids, namely THC. To avoid confusion I will refer to it only as cannabis oil).
Cannabis oil refers to a highly potent extract of cannabinoids from cannabis, especially THC, usually in the range of 40-90% purity (though there are claims of higher purity), in the form of a thick oil that can be taken daily. The same science discussed above applies to cannabis oil as the same cannabinoids are present, only with the oil they are in much higher concentrations. It is due to the increased potency in cannabinoids, specifically THC, that cannabis oil is the most medicinal and beneficial form of the medicine.
The use of cannabis oil became most prominent due to a documentary made by a man named Rick Simpson. The documentary is called ‘Run From The Cure,’ ( the word cure referring to the conventional cures for cancer, like chemotherapy. The documentary focuses on the science of the endocannabinoid system, how to make the oil and what to expect, doctor testimonials, research regarding cannabis’ effect on cancer, and testimonials from patients that have used cannabis oil to successfully cure their cancer.
Another story that is making ground breaking news is a story that is dubbed: Brave Mykayla. It is the story of Mykayla Comstock, a 7 year old girl from Oregon who successfully used medical marijuana, specifically cannabis oil, to fully cure her leukemia.
Additional information on Rick Simpson, Rick Simpson Oil (cannabis oil created using Rick Simpson’s simple method), and how to make cannabis oil yourself can be found on Rick Simpsons personal website: http://phoenixtears.ca/.
Cannabis oil is effective to an unprecedented degree, so says science and the people who have used it successfully to treat their cancer. Unfortunately, unless you are approved to use cannabis medically, it is incredibly expensive and potentially dangerous to procure due to its legal status. Something obviously needs to change, but what can be done? What’s the next step?
*Note: Although it does not specifically contain a discussion on cannabis oil, this exceptional video speaks extensively on the overall science of cannabis’ effects on the endocannabinoid system, presents testimonials from doctors and patients, and discusses various government funded/peer reviewed studies verifying cannabis’ extraordinary effects. It is the video I recommend to anyone even remotely interested in the subject, and is a great introduction to the plethora of research on the issue. It contains the following credible credits:
http://www.knowledgeoftoday.org
Dr. Robert Melamede, Ph.D.
Associate Professor and Biology Chairman
Biology Department at the University of Colorado
CEO and President of Cannabis Science
“Cannabinoids kill cancer cells in many cases, people are not aware of this”
Dr. Manuel Guzman, Ph.D.
Department of Biochemistry and Molecular Biology
Professor at the Complutense University, Madrid, Spain
“Cannabinoids have the effect of inducing death in cancer cells”
Dr. Prakash Nagarkatti, Ph.D. Vice President for Cannabinoid Research
University of South Carolina Columbia Distinguished Professor
“Cannabinoids can be used effectively as anti-cancer agents”
Dr. Sean McAllister CPMC Scientist
California Pacific Medical Center Research Institute http://thesethgroup.org/videos.html
“Cannabidiol inhibits aggressive breast cancers”
Dr. Donald Tashkin, M.D.
University of California, Los Angeles
Emeritus Professor of Medicine
Medical Director of the Pulmonary Function Laboratory
“THC actually has an anti-tumor effect”
Dr. Robert Sterner, M.D.
UCSD General Surgeon
Graduate of Harvard & UCLA
“Marijuana seeks out cancerous cells and preferentially kills them”
Dr. Jeffrey Hergenrather, M.D.
Addiction Medicine Specialist
President of the Society of Cannabis Clinicians
“There are multiple mechanisms of action in which cannabis kills cancer cells”
Dr. Bonni Goldstein, M.D.
Canna Centers, Medical Director
Cannabis Researcher and Scientist
“Cannabidiol has been found to make cancer cells commit suicide”
Dr. Josh Wurzer, Researcher
Laboratory Director, SC Laboratories
Cannabis Researcher and Scientist
“Health benefits attributed to THC is actually because of the CBD content”
What’s the Next Step?
It should now be clear by reading this report that cannabis and hemp remain illegal for utterly irrational reasons that are actually damaging society as a whole. Most importantly, cannabis should not be labeled a schedule 1 substance as it contains, at the very last, a substantial amount of medicinal value. This medicinal effect comes with the added bonus of having little to no danger of addiction, overdose, or biological harm; something that cannot be said about most other substances approved by the FDA. Even aspirin, a substance millions of people around the world pop like candy, kills 1000’s of people every year. Let’s not forget that the most popular pain killer in the world has been found to substantially increase heart attack risk.
A slew of studies…show diclofenac — sold under the brand names Voltaren, Cambia, Cataflam and Zipsor — is just as likely to cause a heart attack as the discredited painkiller Vioxx (rofecoxib), which was pulled from the U.S. market in 2004.
We have so many issues with modern medicine, yet a cheap (free if you grow it) natural, highly effective medicine/pain killer already exists in the form of cannabis. Why is it still only available to less than half the country, and only after jumping through extraordinary loopholes? Even more ludicrous, although medical cannabis users are practicing their legal state right, and moreover, the natural right to peacefully preserve their own lives, they are still labeled by the federal government as criminals deserving up to life sentences behind bars. This is alarmingly unreasonable and irresponsible decision making at best. At worst it is pure foolishness and downright criminal in itself.
Regardless of medicinal comparisons between substances, what is important is that people have as many medicinally effective substances available to them as possible, without interference from Big Brother. As Lynn Zimmer, PhD, former Professor Emeritus at the Queens College, City University, New York explains:
The question is not whether marijuana is better than existing medication. For many medical conditions, there are numerous medications available, some of which work better in some patients and some which work better in others. Having the maximum number of effective medications available allows physicians to deliver the best possible medical care to individual patients.
We recognize the legal hurdles and the hardships faced by patients fighting for the simple right to take a safe, proven to work medicine, but what is the next step? What must occur to end the madness?
The next step is to step out of the historical shadow of basing medical and political decisions on myths and rumors. More unbiased research needs to be performed on the effects of cannabis on each and every part of the human body and psyche. The DEA, FDA, and NIDA have made further legitimate research an ongoing uphill battle.
A pro-marijuana group lost its legal battle this week when a federal appellate court ruled that marijuana would remain a Schedule I drug, defined as having no accepted medical value and a high potential for abuse. The court deferred to the judgment of federal authorities, quoting the DEA’s statement that “the effectiveness of a drug must be established in well-controlled, well-designed, well-conducted and well-documented scientific studies…. To date, such studies have not been performed.
But guess who bears responsibility for the studies the court claims are not being performed? The DEA itself, which through its ultra-tight restrictions on marijuana has made it nearly impossible for researchers to obtain the substance for study, as well as the National Institute for Drug Abuse, which controls the availability of the tiny quantity of research-grade marijuana that is federally approved for production.
In response to the DEA’s actions against sensible substance users, the LA Times accurately labeled the DEA as
a terrified and obstinate toddler when it comes to basic science.
Probably the most ridiculous aspect of the FDA’s behavior is that they approve of multiple synthetic cannabinoids which precisely mimic natural cannabinoids found in cannabis, especially THC. The only difference is that they and the pharmaceutical companies can add a few substances to the cannabinoid, call it a cocktail, and turn a significant profit on people in desperate need for something that works. So, synthetic cannabinoids which can be patented and sold at exorbitant rates are legal but naturally grown, free medicine containing the same exact cannabinoidal actions, as well as a wider range of medicinal benefits remains illegal. It doesn’t get much more hypocritical or shameless than that.
We have the ability to breed specified strains of cannabis, and create particular synthetic cannabinoids to meet the precise needs of patients. This incredible opportunity to create safe, effective, highly personalized medicine is stifled at the federal level, despite opposition from a majority of the US public.
The fact remains that Americans love cannabis. A recent survey of over 85,000 people revealed that at least 42% of Americans have tried cannabis. This is extremely surprising as only 20% of people in the Netherlands have tried cannabis, a country with extremely lax cannabis laws.
A second poll found that nearly 50% of Americans support legalizing cannabis, while 83% favor legalizing medical cannabis. Cannabis is such an American pastime that companies are planning to install cannabis vending machines in Washington and Colorado. Does this mean that 42% of Americans should be in prison, and 83% of Americans should be on the wanted list for supporting an act listed as a felony?
(*Percentages reflect any cannabis use during a person’s life for the stated ages in the stated year.)
http://www.dope-smoker.co.uk
Canada: 44.5% (ages 15+ in 2005)
United States: 42.4% (ages 14+ in 2002-2003)
New Zealand: 41.9% (ages 16+ in 2004-2005)
Denmark: 36.5% (ages 16-64 in 2005)
Australia: 33.5% (ages 14+ in 2007)
France: 30.6% (ages 15-64 in 2005)
United Kingdom: 29.6% (ages 14+ in 2004)
Italy: 29.3% (ages 15-64 in 2005)
Spain: 28.6% (ages 15-64 in 2005-2006)
Chile: 26% (ages 12-64 in 2009)
Germany: 24.5% (ages 18-59 in 2003)
Netherlands: 22.6% (ages 15-64 in 2005)
Czech Republic: 20.6% (ages 18-64 in 2004)
Scotland: 20.5% (ages 16-64 in 2004)
Austria: 20.1% (ages 15-64 in 2004)
Millions of people worldwide use cannabis for an endless list of reasons. Besides using it as a medicine, people all over the world responsibly use cannabis to experience:
Why are the DEA/FDA stalling? They raid innocent people’s homes, destroying families and jailing individuals for hyperbolic amounts of time. They go to all this effort to rid society of non-violent, victimless crimes. All this fear and war over a substance that they admit is beneficial (ie. allowing synthetic cannabinoids to be used medicinally and still sending medically grown cannabis to individuals). This is explicitly hypocritical and undoubtedly insane.
If the DEA/FDA are truly concerned over Americans’ safety, why are they not going after the truly dangerous substances. Research routinely finds that cannabis is strikingly safer than alcohol and tobacco within every measurable facet.
According to a 2006 United Kingdom government report, using cannabis is much less dangerous than tobacco, prescription drugs, and alcohol in social harms, physical harm, and addiction.
The scheduling system is nonsensical and has no clear logical basis for the large majority of listed substances.
Another important point is that through the legalization of cannabis, the economy could be booming! Here is a list of some examples of how cannabis legalization has already positively affected the economy, and how further legalization will improve the economy in the future:
Tobacco companies have the land to grow it, the machines to roll it and package it, the distribution to market it. In fact, some firms have registered trademarks, which are taken directly from marijuana street jargon. These trade names are used currently on little-known legal products, but could be switched if and when marijuana is legalized. during the run up to the 2010 election in which marijuana legalization was on the ballot in California, Altria took control of the web domain names AltriaMarijuana.com and AltriaCannabis.com. For those not in the know, Altria is the parent company of Phillip Morris, the manufacturer of Marlboro, Players, Benson & Hedges and many other popular brands of tobacco cigarettes.
We calculate that a reduction by one-half in the incarceration rate of non-violent offenders would lower correctional expenditures by $16.9 billion per year and return the U.S. to about the same incarceration rate we had in 1993 (which was already high by historical standards). The large majority of these savings would accrue to financially squeezed state and local governments, amounting to about one-fourth of their annual corrections budgets. As a group, state governments could save $7.6 billion, while local governments could save $7.2 billion.
Cannabis has the potential to change everything for the better. It could also help alleviate the health care crisis as Americans would be able to grow their own highly effective medicine. Let’s not forgot about the multitude of uses for hemp. It’s no wonder so many industries are lobbying against cannabis and hemp legalization including:
Vote! Voting is one of the best ways to enact change. It’s how Washington and Colorado were able to finally legalize cannabis.
Talk to your representatives. Send an email to your house representative and your state senators. Let them know how you feel, and how you think they should vote.
Do your own research. Alter your perceptions so that they are founded on evidence and scientific data.
Spread the world. Share this report or other relevant information you find and help educate others. Don’t be afraid to talk to people and tell them about what you’ve learned.
Don’t give up: people’s freedom and lives are at stake!
Final Thoughts
I would like to take the time to point out that this report’s aim is to argue why cannabis should be recognized as a medicine, and to thoroughly point out how incredible it is that it is not. Although I am admittedly in favor of it, I am not arguing for recreational use. Medicinal availability and options that work are the priorities here.
Virtually everything we encounter in life can be abused and unhealthily depended upon for happiness, be it video games, work, sex, masturbation, food, television, coffee, nail biting, reading, or even heavy metal. If you are going to use cannabis recreationally, use it responsibly, and don’t abuse it to the point of dependence. A relatively small amount of very heavy cannabis users do report withdrawal symptoms when attempting to stop smoking, but symptoms are extremely mild and usually involve difficulty sleeping, loss of appetite, and moodiness for 1-7 days. Regardless, this shows that despite the safety, a socially harmful dependence remains possible, as is the case with everything in life. Remember, cannabis should be used in moderation (or as directed by your physician if you are using it medicinally). Moderation is the key to happiness and health.
To put it simply, cannabis is not for everyone, but that does not mean people who safely and peacefully ingest cannabis should be seen as criminals.
A paradigm shift in information availability and critical thinking is occurring in humanity, an ubiquitous evolution on a global scale. We are growing out of outdated traditions. More and more often we are basing our decisions on fact and evidence, rather than on opinion and stipulation. My hope is that by reading this report you will be sufficiently equipped with the proper information to understand an aspect of the changes that are occurring all around you. Become part of the solution. Don’t just listen; wonder, research, evaluate, consider…and be always growing.
Warning: this article should not be read within proximity to sandpaper or pumice rocks as there is a high likelihood of sanding down one’s skin in terror. This one gets gross, kiddies.
One of the many benefits already seen since the inception of the Human Microbiome Project in 2007 is the outrageous discovery that only 10% of our body is human.
What kind of madman rant are you going on this time, Qwizx?
As it turns out, crazy as it may sound, the overwhelming majority of cells within/out our person are bacteria. In fact, we are a staggering 90% non-human. Swimming amidst the estimated 10 trillion cells constituting your selfness are something like 100 trillion individual little critters that call your life-fluids home. In a microscopic landscape of terrain, legions of monsters are swathing, swarming, warring, breeding, breathing and all-out taking over the slabs of meat we self-reference as “I.”
100 trillion is a big number, maybe too large for a human mind to fathom, so instead, let’s imagine it this way: There are currently 7,000,000,000 people in the world (that’s billion, with a B)… There are 14 THOUSAND times that many (our current planetary population) bacteria wiggling inside you this moment, Jacuzzi-ing in your tear-ducts as you read this. When I say bacteria, by the way, I mean these things (thank you, electron microscopes)…
Cluster of E. Coli sipping margaritas by the lake of sulfur in hell, or…
Life always finds a way, just not necessarily humanoid life. A genomic sequencing study has recently discovered high numbers of hydrothermal vent eubacteria on prosthetic hip joints. This wouldn’t be a big deal, considering the plethora of ghouls infesting people, accept hydrothermal vent eubacteria are a species once thought only to live in the blackness of the ocean’s depths(you know, cause surviving on uranium isn’t scary enough).
(below) At Steve’s liver for the weekly orgy and ritual-sacrifice (BYOB)
By no means is this exclusively shiver-inducing news. Like when Copernicus realized the earth revolved around the sun, this is a “discovery,” meaning it was always true, just now it’s news to us. No need for mass panic, cause this is how it’s supposed to work, and always has. However, there are some interesting implications:
Hurray, no more lonely Saturday nights!
Imagine our bodies, now, as a planet onto themselves, where bacteria pay their property taxes, vote, and even take their kids to little league in the small intestine. We humans are not individuals, but a collective, a civilization or a conglomerate, united in a symbiosis where each individual creepy-crawly plays his part on the whole. Sure, just like in human civilizations, there are the equivalent of warring gang factions, and like we always do, these sparse rebels gets all the focus (I’m looking at you, gonorrhea.), but our microscopic brothers and sisters are absolutely essential to our continued existence.
If we’re like a corporation, hell yeah, I get to be the CEO.
Not quite. Sorry. We’re more like the semi-dipshit boss wrapped around his employees’ fingers. The sneaky scallywags just let us think the best ideas are ours so we can save face; the germs are in charge. Through the clever excretion of chemicals, our fuzzy little friends manipulate our lives in almost every conceivable way, from our health to straight up mind-control. However, don’t panic; it’s less like “Invasion of the Body-Snatchers,” and more like the Futurama episode where Fry eats the vending machine egg salad and becomes an Ubber-Fry.
The NIH’s Human Microbiome Project plans on cataloging the entire human microbiome, or metagenome, and thus far only approximately 1% of this microbiota has been characterized and identified. They’ve just begun to peak into the Pandora’s box of possibilities from our neighbors to the nano, so, I don’t know about you, but I’ll be keeping my fingers crossed for sensory enhancing super parasites.
By all means, keep washing your hands, but these guys are unavoidable. See that cute fella hiding in the upper-left corner of this close-up of dust (below), the Kraken-lookin spawn of Lucifer posing for a cameo in your nightmares? He’s everywhere.
The issue of income inequality in the United States has again crept into the blogosphere through a viral video created by user politizane using data from Michael I. Norton and Daniel Ariely. It attempts to illustrate how far off the actual levels of inequality are compared to what people think is the reality and what they believe is the ideal distribution of wealth. Its creator then implicitly implores the viewer to think of ways to end this injustice by flattening out the perceived malapportionment.
My first response to the largely non-issue of inequality is a very blunt “So what?” As income inequality has increased, the standard of living has also surged to the point where it’s almost meaningless to talk about “the poor” in America these days. However, more important than the message of the video itself is its tacit endorsement of leveling the distribution of wealth in America, a proposition that is largely impossible without forcefully taking it away from the Haves.
Income inequality in the United States simply isn’t scary or even an undesirable condition. In fact, it has been one of the drivers of innovation in this country, a phenomenon that helped everyone become wealthier as technological advances eventually trickled down to even the poorest in our society. The US during the Gilded Age in the late 19th and early 20th centuries had large amounts of inequality, personified by mega-rich barons of the day like Vanderbilt, Carnegie, Ford and Rockefeller. Despite this, the quality of life improved dramatically for everyone regardless of social standing. In 1850 the average life expectancy in the US was 39.5. By the end of the century it had risen to around 49 and was nearly 60 by 1930.
This boost in the standard and quality of life was accompanied with a transformational technological boom that dramatically altered the way people lived. Even completely ignoring the end of slavery and the obvious progress blacks made towards racial equality, is there anyone who really thinks that 1850 was a better time to be born than in 1900? And to think, all of the cultural, financial and industrial advancement occurred in spite of—or perhaps because of—wealth inequality. The video gives another example: the narrator states that in 1976 the top 1% had 9% of the nation’s wealth, compared to 24% today. Considering how much “fairer” the country was back then, how many of you would rather be living in 1976? Hands? Anyone?
Another problem with the video lies in its fallacious depiction of poverty in America. When illustrating the actual distribution of wealth, the narrator describes the poorest Americans as being “down to pocket change.” While there is poverty in the US and I do not intend to denigrate the people living through tough times, the fact of the matter is that poverty in America looks dramatically different than actual poverty.
Poverty is when meeting the basic needs of food, shelter and clothing is a constant struggle. People living in war-torn Afghanistan are impoverished, as are those that live in the favelas of Rio de Janeiro or the slums of Jakarta. Most poor people in the US are only poor in relation to rich people, because thankfully this type of extreme poverty is exceptionally rare in America.
The Heritage Foundation produced a very illuminating study of the realities of the more than 30 million Americans who are defined as “in poverty” by the Census Bureau. Using figures from 2005, they listed household amenities and documented what percentage of poor households separately owned each item. Over 60% owned a cordless phone, clothes dryer, at least one DVD player, more than one television AND cable/satellite service, at least one VCR, air-conditioning, microwave, stove, oven and refrigerator. Of these poor households, 38.2% had a personal computer, about 30% had Internet access and over half had a cell phone, all astonishing numbers.
Is it really appropriate to call someone poor if they can sit in their air-conditioned house and sip a cold, refrigerated beverage as they surf the net? Honestly, if 17.9% of “poor households” own a big-screen TV, then perhaps it’s time to redefine what being poor actually means.
The implications of the video and the sentiment behind it are also disturbing. Over somber music, the narrator details the actual distribution of wealth in the nation and makes pleas “to find something that is fair for hardworking Americans.” Clearly, politizane thinks wealth inequality is unfair and harmful, a societal ill that needs rectifying.
The really scary part is how some people plan on “fixing” the fiscal unbalance. France has already created a 75% upper tax rate on income over one million euros that has led some to flee the country in order to keep their money. Switzerland has also recently made it illegal to pay a CEO too much, with a penalty of up to three years in jail.
Raising taxes on the rich and penalizing “excessive” compensation smacks of petty wealth envy, punishment for the crime of having more money than someone else. The top 1% already pays 37% of federal income taxes, and the top 5% pay 59% of the total. Just how much more should they have to pay in pursuit of “fairness?”
Politizane’s video does mention the “Dreaded Socialism” and how it’s unnecessary to fully implement that failed philosophy. However, any attempts to redistribute wealth from Washington must, at their core, be socialistic. Confiscating wealth in order to be more equitable is inherently immoral, especially when Washington spends so recklessly and inefficiently that they give drunken sailors a bad name. After all, trillion dollar deficits are the new norm and Congress has failed to pass an actual budget three years in a row, with Obama’s last attempt being voted down 99-0 in the Senate.
Trying to reallocate wealth through higher tax rates, salary caps, or any other conceivable method is hazardous, unethical and largely pointless. Rather than reflexively freaking about income inequality, politizane and others who share his concerns should take a deep breath and realize that it simply isn’t the great boogeyman that they fear it is. In fact, it actually helps drive the standard of living up for everyone, because as the rich buy products that only they can afford (e.g. cellphones in the ’80s), soon enough the technology is cheap enough to positively influence all of us.
Income inequality is nothing more than a red herring meant to inflame wealth envy into hatred of the rich. By ignoring this myopic view of society and realizing that other people’s wealth is no one else’s business, hopefully we can continue to enjoy the unprecedented advances in technology that make the Internet Age such a marvelous and truly progressive time to be alive.
Drones give law enforcement agencies unprecedented abilities to engage in surveillance and intrude on people’s privacy
Dave Norris, a city councilman in Charlottesville, Va. says:
I don’t mean to sound conspiratorial about it, but these drones are coming, and we need to put some safeguards in place so they are not abused
With the looming threat of overpopulation, is it a question of morality to set these drones afloat that is, for the time being, forcing them to stay grounded? Is this simply one more step towards total control that is part of a New World Order scheme? Or is this simply a cost effective way of handling crimes in a technologically advancing society? Like it or not, THE DRONES ARE COMING!
The rate of obesity in America and the West is just as much in an incline as low fat and low carb diet fads. Do you know someone who successfully lost weight recently from a strictly low fat diet?
Obesity and Low Fat Diets
Low fat diet fads started to appear in the 1980s, but the obesity rate then was nowhere close to what it is now. Also, after the introduction of low fat diets, the rate of obesity did not fall, rather it increased. So where did we go wrong?
Food Portions
For the past 20 or 30 years, ads for low fat food products started to proliferate the market at an alarming rate. What also increased at a steady pace was the average American food portion. Furthermore, there was a rapid replacement of fat with carbohydrates, including sugars. For the food companies to be able to produce products that people would salivate over, this was a necessary step. This is a step backward in the fight against obesity. Let’s not forget that the food companies don’t have our best interest in mind. The amount of ingredients also doubled, or even tripled for some items, such as JIF peanut butter. Try to compare the ingredient list between the regular JIF peanut butter and the low fat version.
Enter Low Carb Diets
After seeing that obesity was far from being solved by a low fat diet fad, we turned to a new approach; limiting our carbohydrate intake. We have realized that we are consuming way too many simple and processed carbohydrates. Carbohydrates make up the majority of a Westerner’s diet. We saw the rise of such diets as the Atkins diet. There are countless forms of low carb diets out there. This seems to have partially solved the problem as lowering overall carbohydrate intake does decrease the rate of obesity to a certain extent (many studies have even linked low carb diet with blocking the effects of aging!). Despite many successful cases, the West is still fighting obesity more than ever. Perhaps there is a crack in this low carb diet that needs to be patched up.
Successful High Carb Diets
A local tribe in Papua New Guinea called the Kitavans have a diet that is comprised of 65% carbs, 17% saturated fat, and high fiber, yet their obesity rate is at 0%. Literally no obesity at all has been reported thus far. They are also not prone to strokes, diabetes, nor heart disease. Their diet mainly consists of starchy root vegetables, fruit, some fish and meat, and coconuts. Food is also abundant and they don’t suffer from scarcity.
The Machiguenga people, local to Peru, also have a diet that is high in carbohydrates and fiber. Their diet also consists of mainly root vegetables, fruits and nuts. Meat and fish are eaten in low amounts. These people also don’t have reported cases of obesity.
The Mexican Pima Indians have a diet that roughly consists of 62% carbohydrates, high fiber intake, and 25% saturated fat. There is a 7% obesity rate in males, and 20% obesity rate in females. Incidence of diabetes is at 7%. Their diet mostly consists of beans, wheat-flour tortillas, corn tortillas, and potatoes.
Just across the border, the Arizona Pima Indians have a diet that consists of 49% carbohydrates, 15% protein, 34% fat, and more than 10% of it is saturated fat. Even though they consume less carbohydrates, the obesity rate in males is 64%, and in females it is 75%. Over 30% have been reported to have diabetes. The big difference between the two people is in their diet. The Arizona Pima Indians consumed fried breakfasts, processed meats, hamburgers, pork chops, beans, white bread, flour tortillas, fried or baked dough, cereals, canned foods, and fruit juices.
The Culprit: Carbohydrate Density
According to the National Institute of Health, the diet of these people is closely tied to the diets of people in the Paleolithic period. The main trait that these people share is consuming cellular carbohydrates as opposed to acellular ones. Foods that have living cells such as fruits and vegetables contain the carbohydrates inside the cells themselves. The maximum density of carbohydrates that a cell will allow is at 23%. Most of the cell’s mass is comprised of water. When digesting these sources of carbohydrates, it also takes time for the stomach to break up the cellular walls and take in the energy from the carbs.
Acellular carb sources, on the other hand, are very simple in form and contain no cellular walls. There is nothing between them and the stomach microbiota. They are easily taken in by the body and swiftly used. These include all wheat products, grains, and sugars. These are also what currently dominate the ingredient lists in Western diets. All things being equal, macronutrients, amount of carb intake, calorie intake, etc.; it is the foods with the higher carb density that relate to the promotion of obesity. The chart in the beginning of the article shows foods (in grey) that are dominant in the modern diet, and the ancestral diet (white).
The discussion about carbohydrate density and its relation to obesity will continue in a follow up article, but for now, the main point that I am trying to summarize is: stick to foods that have a lower carbohydrate density, and you will be more than likely to prevent obesity.





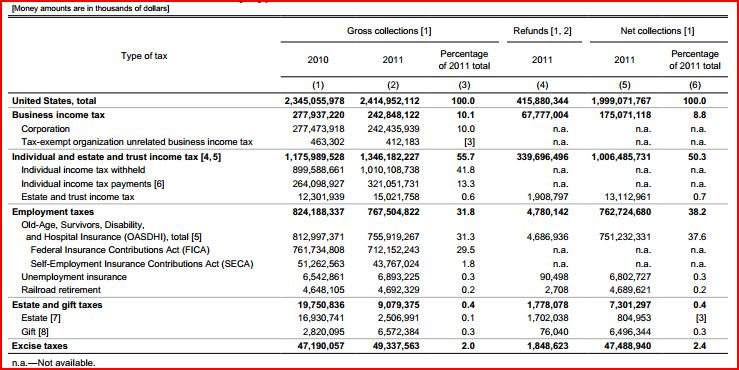
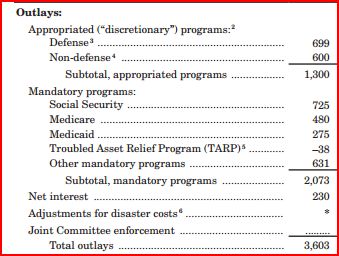




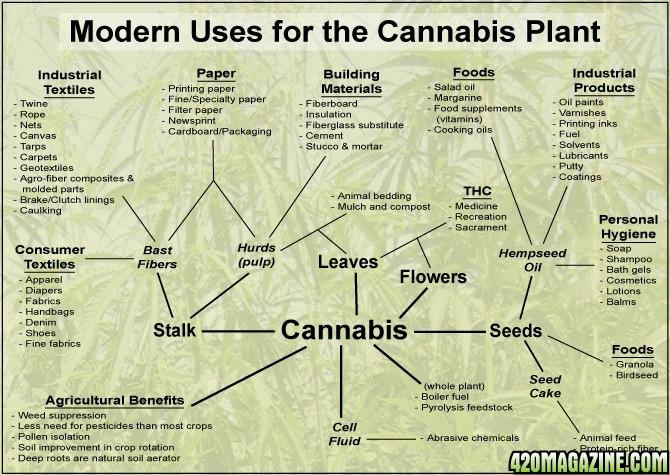


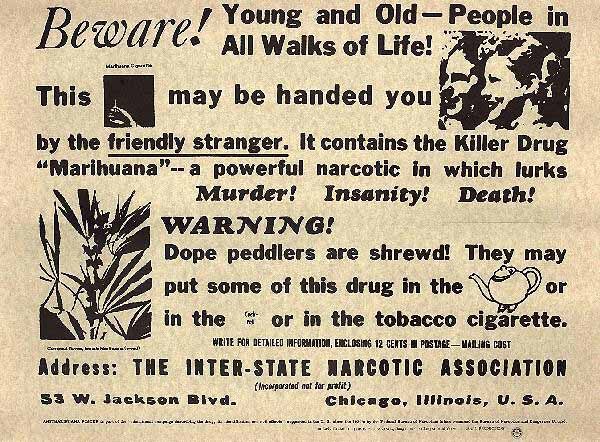

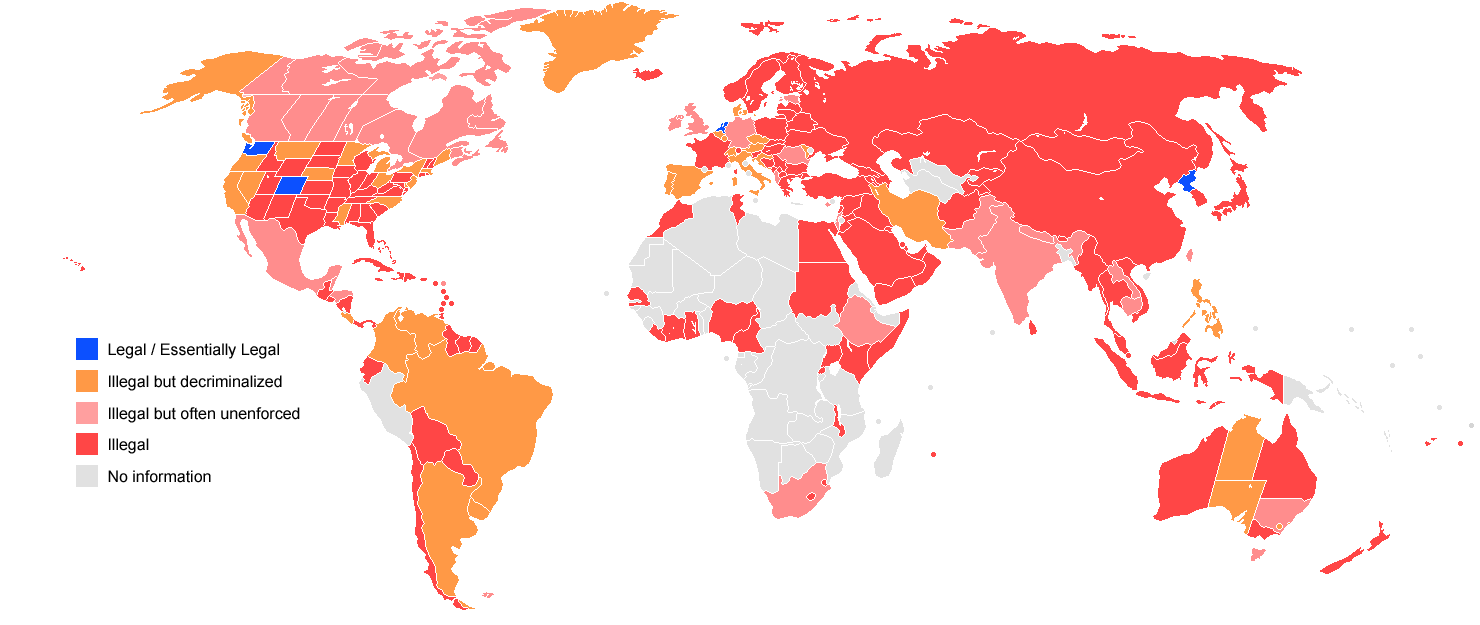

 In an interview with Barbara Walters concerning cannabis legalization in Colorado and Washington President Obama said:
In an interview with Barbara Walters concerning cannabis legalization in Colorado and Washington President Obama said:

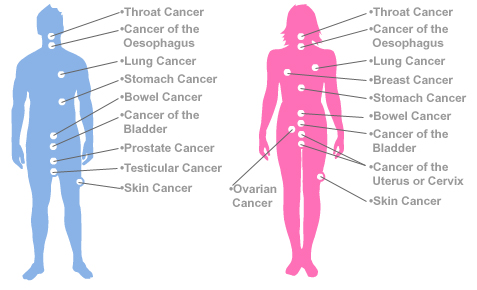
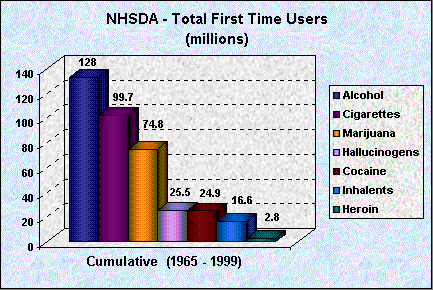
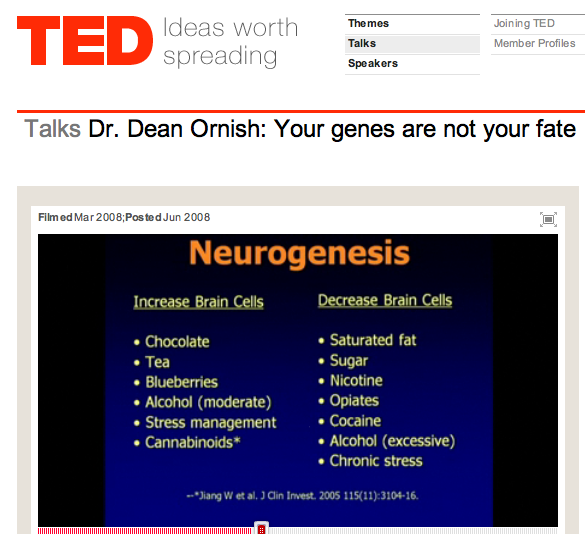

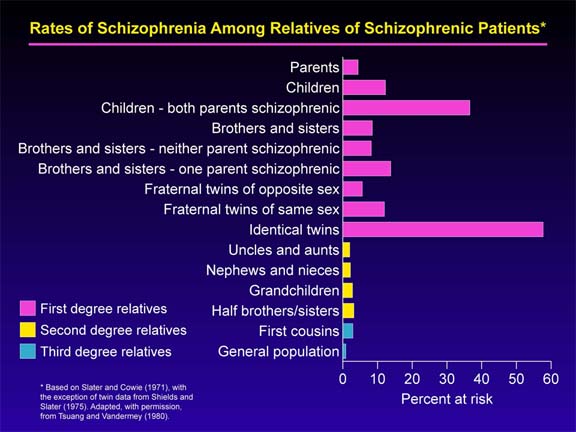




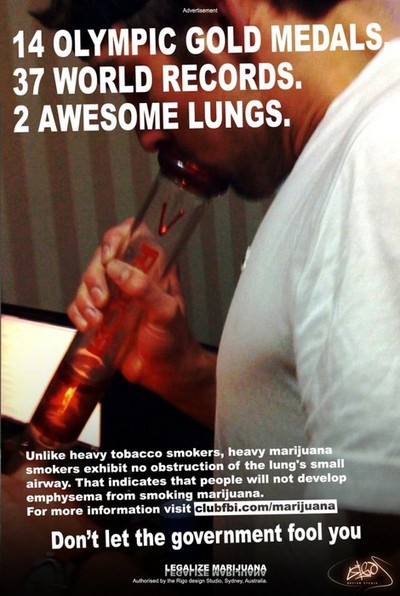
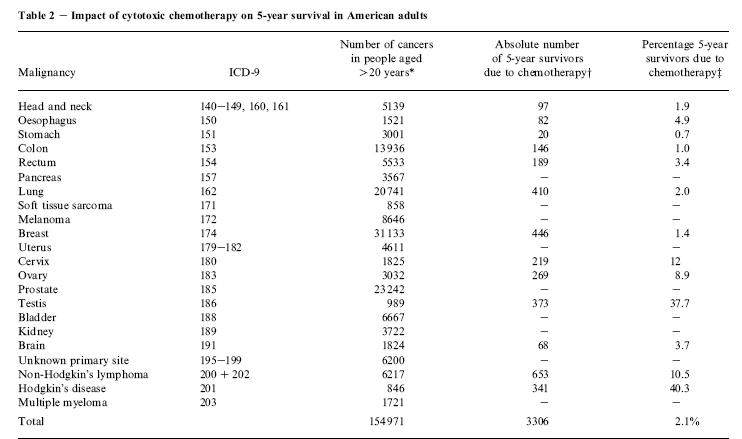

 We have so many issues with modern medicine, yet a cheap (free if you grow it) natural, highly effective medicine/pain killer already exists in the form of cannabis. Why is it still only available to less than half the country, and only after jumping through extraordinary loopholes? Even more ludicrous, although medical cannabis users are practicing their legal state right, and moreover, the natural right to peacefully preserve their own lives, they are still labeled by the federal government as criminals deserving up to life sentences behind bars. This is alarmingly unreasonable and irresponsible decision making at best. At worst it is pure foolishness and downright criminal in itself.
We have so many issues with modern medicine, yet a cheap (free if you grow it) natural, highly effective medicine/pain killer already exists in the form of cannabis. Why is it still only available to less than half the country, and only after jumping through extraordinary loopholes? Even more ludicrous, although medical cannabis users are practicing their legal state right, and moreover, the natural right to peacefully preserve their own lives, they are still labeled by the federal government as criminals deserving up to life sentences behind bars. This is alarmingly unreasonable and irresponsible decision making at best. At worst it is pure foolishness and downright criminal in itself.
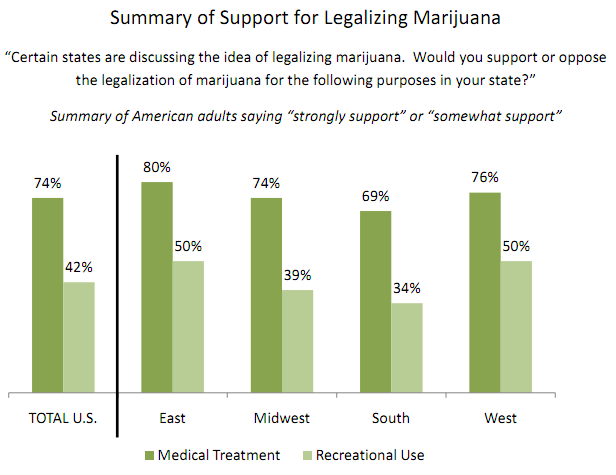
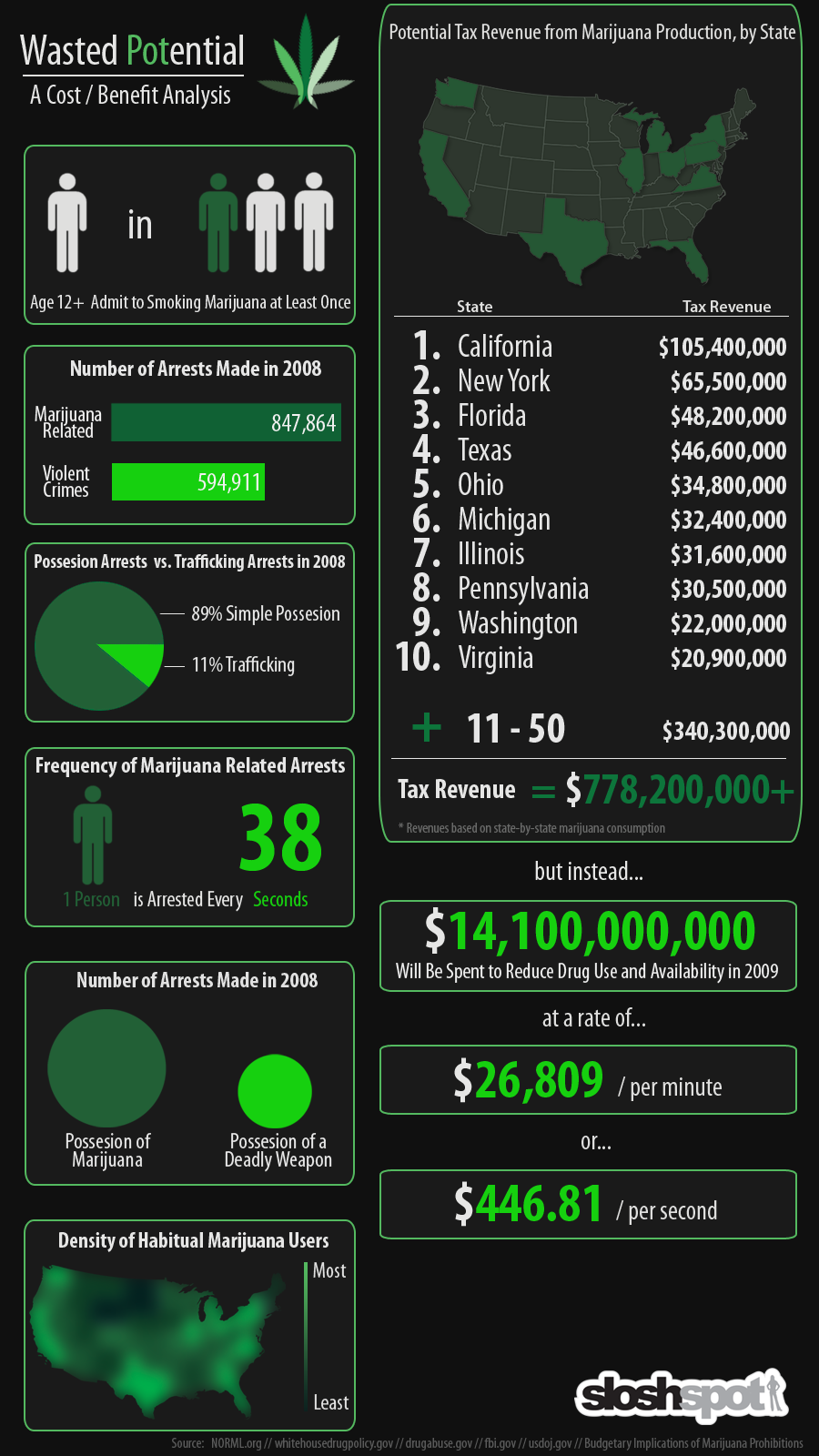



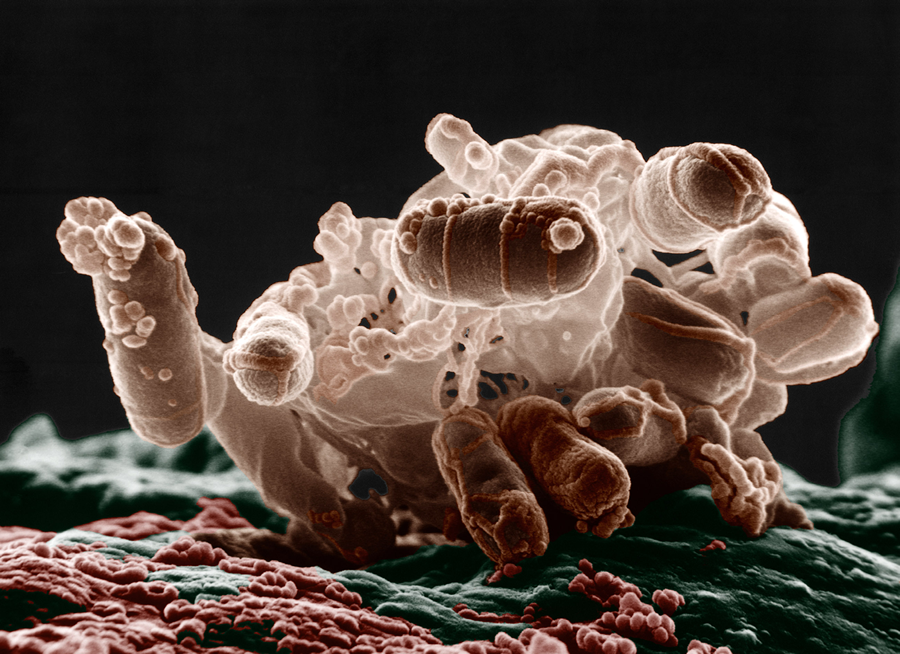

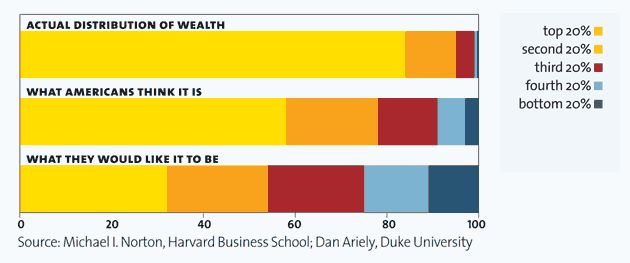



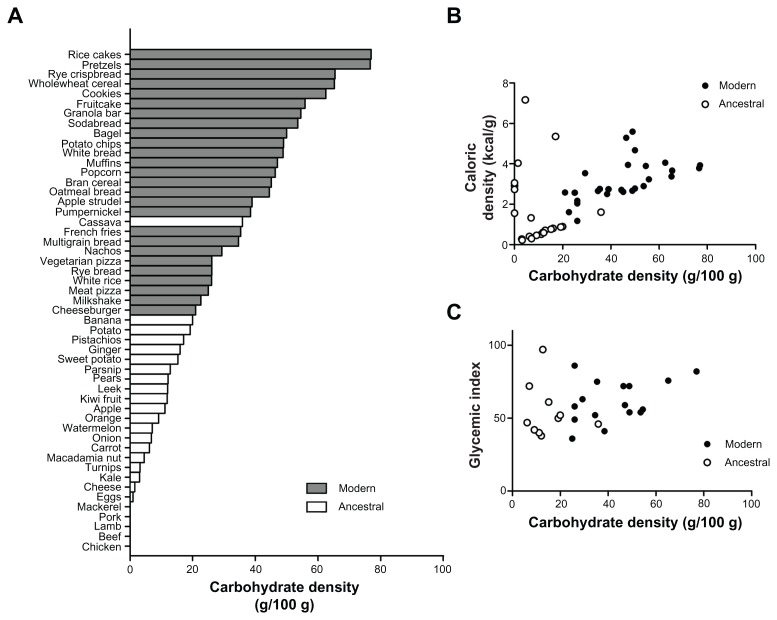

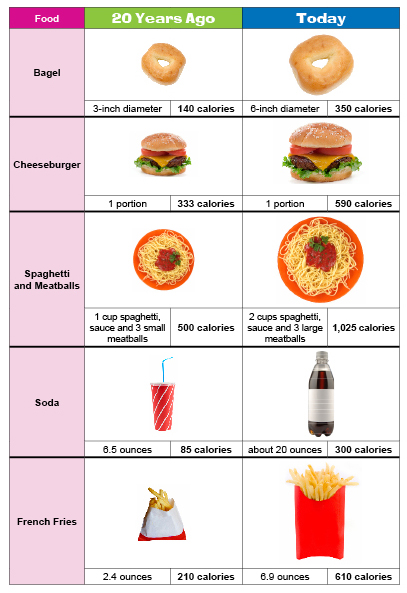







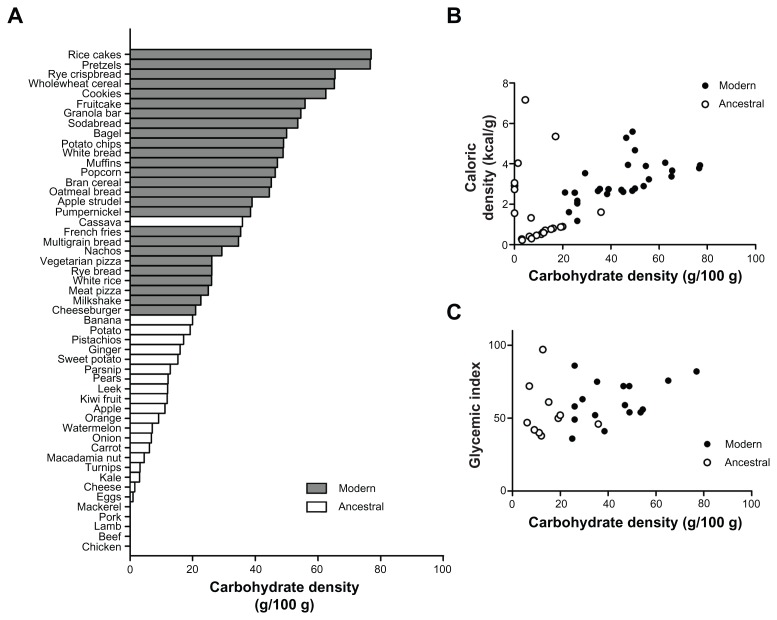

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}